
Today’s discussion is going to be a little different from my usual teaching spiels and is focused more-so at clinicians – physicians, pharmacists, NPs, PAs, etc – and tips and tools that you can use to help get your patients blood pressures controlled.
It’s nothing new that HTN is extremely prevalent in the USA and one of the factors that heavily contribute to ASCVD morbidity and mortality every year. An estimated ~120 million patients in the US have HTN, and 94.9 million require medication. For those who are on medications, we still see 77.5% of these patients uncontrolled. Let’s say that again:
In patients with HTN in the US on medications, more than 3 out of 4 patients are still uncontrolled and not at goal.
There is clearly a huge unmet need to help these patients get their blood pressure controlled. Besides reducing outcomes and deaths in these patients, as clinicians working with this patient population – you probably are also very familiar with the amount of time, repeat visits, emergent hospitalizations for hypertensive crises these patients require.

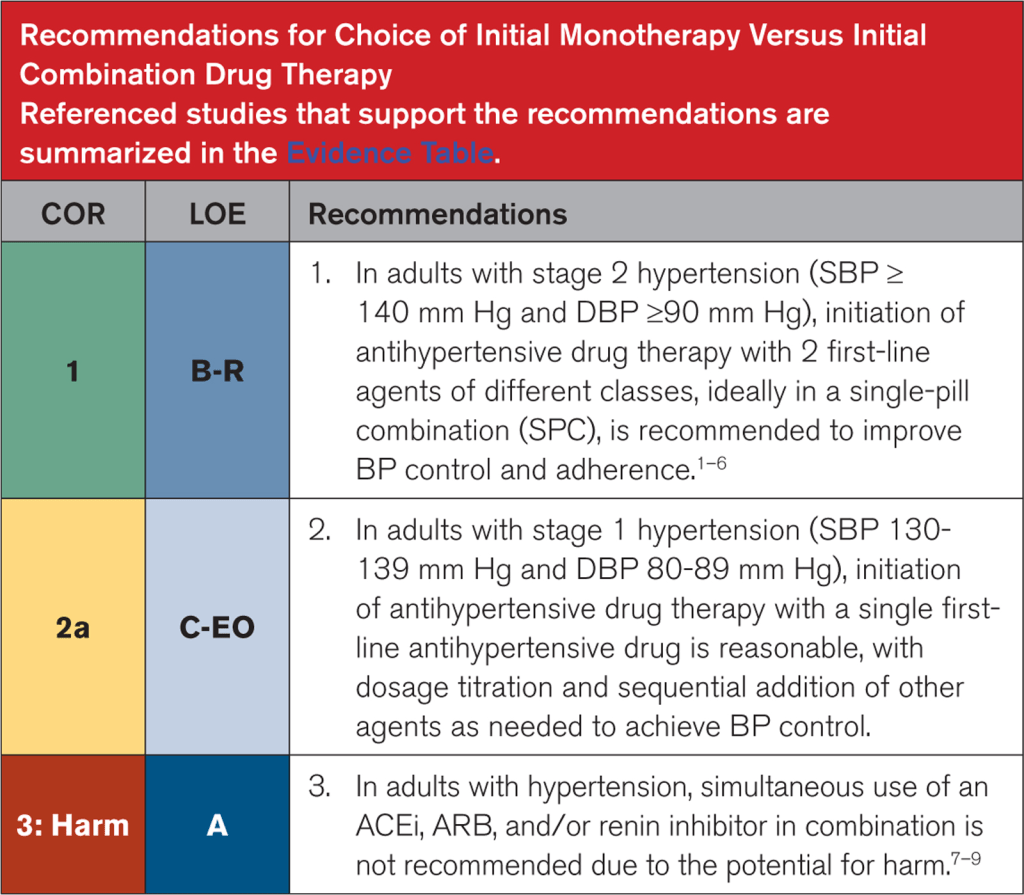
The latest 2025 AHA/ACC/multi-society hypertension guidelines have a new recommendation pushing towards the use of single-pill combination therapy for all patients with stage 2 hypertension.
A big push and change that we see in the latest rendition of the new American hypertension guidelines is this push for the use of single-pill combination (SPC) in patients who present with stage 2 hypertension (defined as SBP ≥140 mm Hg and DBP ≥90 mm Hg – in other words, a big chunk of patients we might see in clinic), ideally with 2 first-line agents of different classes.
Now – this idea is not novel – Europe has been recommending this since the 2018 ESC/ESH guidelines (I swear, ESC is always 2 steps ahead of the US…even their guideline figures are cuter).
Investing the time upfront to making sure your patient can get access to their SPCs is time well spent. We’ve all been there – a super uncontrolled hypertensive patient who you’ve ever so slowly gone up on their antihypertensives, but every time they come in, their BP is SBP is in the 160s or worse. SPCs can not only enhance efficacy but also adherence. Investing the time to make sure your patients can get their medications helps prevent back to back clinic visits for sometimes months on end, leaving you more time to focus on other things (all while improving patient outcomes).
The Data: Stepwise Approaches and SPCs
There are no RCTs looking at stepwise approach vs initial combination therapy. However, I think often what a lot of us worry about when adding more than one medication at a time is side effects. We always want to do no harm. How do patients tend to do when starting SPCs?
Well, the data shows us that combining anti-hypertensives with complementary mechanisms not only enhances BP lowering but also might reduce side effects.
Adding a RAS blocker with a thiazide can reduce the incidence of hypo- or hyper-kalemia; combining an ACEi/ARB with a DHP CCB can reduce the incidence and severity of peripheral edema. The latest guidelines say it very well:
“Combination therapy is more effective, efficient, and consistent in lowering BP and improves adherence when using an SPC compared with stepped-care therapy.”
Medications can transform patients lives and prevent terrible outcomes…but only if our patients can get access to these medications. It’s great that the US has finally caught up with recommending these meds, but how does one go about implementing these meds? Some questions that might come up:
What combinations of antihypertensives are even available? Are they generic? How much do they cost? Is there a way to easily find out if we can get these meds at a cheaper cost?
With this new push on this side of the pond, I wanted to share some useful and practical tools that you can utilize to help make sure your patient gets access to these medications. I am not sponsored by any of these resources and am just truly sharing them because I find them helpful. Let’s get into it.
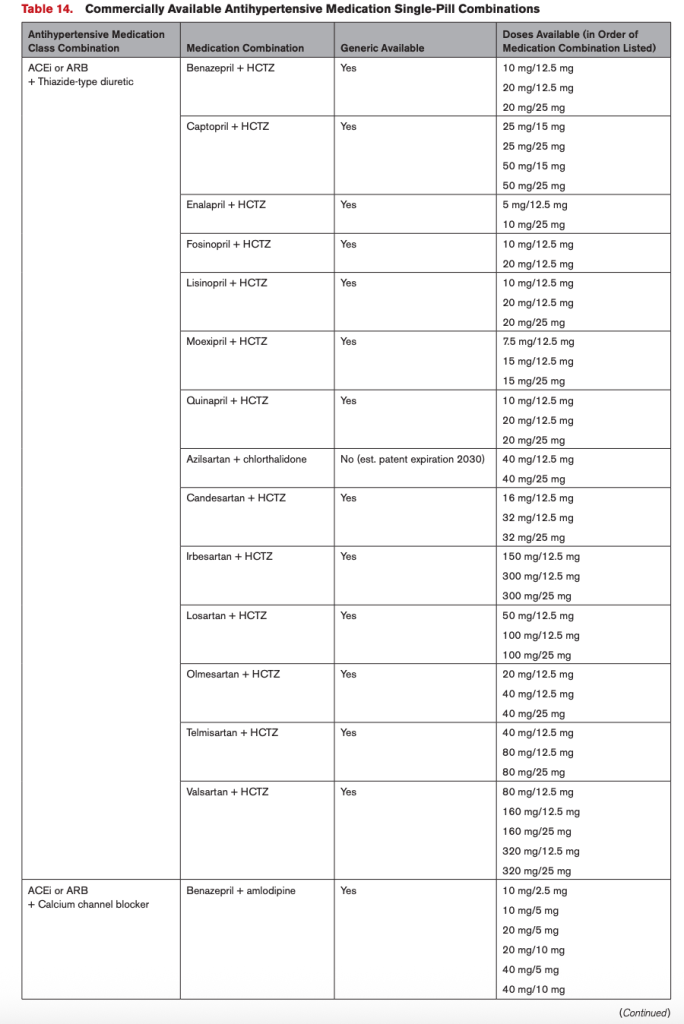
Question #1. I’ve decided I might want to use an SPC in my patient. Now – what the heck do I prescribe? What combinations are even out there?
Cue the updated 2025 AHA/ACC Hypertension Guideline. These people seriously thought it through and made a fantastic resource table. Table 14 of the guidelines have already done that work for US-based providers (see below for a semi-blurry screenshot)

Question 2: Now that I know what SPC’s are available, what about their pricing for my patients?
Pricing is always somewhat annoying to figure out, as every patient has different insurance plans and supplemental plans and blah blah blah. The tools I am going to offer today are independent of insurance (in other words, your patients can get these medications at this rate even if they don’t have insurance). These resources will also provide some references to what the normal out-of-pocket costs would be retail. Unfortunately creating some sort of comprehensive spreadsheet of pricing would not be effective since prices are constantly changing – so the best way to look into prices is looking at pricing in real-time. Below is what I recommend:
- Use the GoodRx App.
GoodRx is a free mobile app and website that helps Americans save money by finding them the lowest cash prices on medications. They offer discounted rates on many medications, independent of insurance. If your patient does have insurance, and their copay is lower than GoodRx, then there is no need to use it. GoodRx will not lower your patient’s copay for medications if they are commercially insured. However, if the GoodRx price is lower than your patient’s copay, then they should forgo using their insurance and simply use the GoodRx code to pay an out-of-pocket cash price. Because they are not using their insurance, this will obviously not be applied to their deductible, if they have one.
GoodRx has both a website that you can use, or an app. I really recommend using the app, especially if you actively see patients in clinic since it is way faster and user friendly to use.
Once you download the app, you can make an account as a healthcare provider. There are some handy tools on here:
- You can search by your medication. When you search for your medication, it’ll tell you what the retail cost (without coupons), and what the GoodRx price is at different pharmacies, and then in general. You can also “bookmark” your medications. In the example above, I searched for enalapril-HCTZ. It defaults at 10/25 mg 90 tablets and lets me know that retail price is anywhere from $40-90 out of pocket. By using the GoodRx coupon, I know that my patient can get the combo pill from Walmart right now for around $30.
- Once you’ve searched a medication, there is a way to easily see other options in that therapeutic class. In the example above, I initially searched for enalapril-HCTZ. You can then look at other meds in the ACEi/thiazide class.
- Once you are on a particular medication, you can play with some options like changing the dose or quantity of the medication. For example, if you need 180 tablets, you can input this to see what the updated price will be.
- How it works: When you click on the price, you will get a screen (see above) with codes for the pharmacy team to input at the pharmacy. Your patient should present this information to the pharmacy staff when they go to pick up their prescription. You can also share this information quickly with your patient or others by selecting the “text” or “email” options.
- If you go to your home page, you can see all of your bookmarked medications. I’d recommend adding the SPCs to your bookmarks so you can quickly see their prices while prescribing, instead of having to type in each separate medication every time.
2. Check out Cost Plus Pharmacy
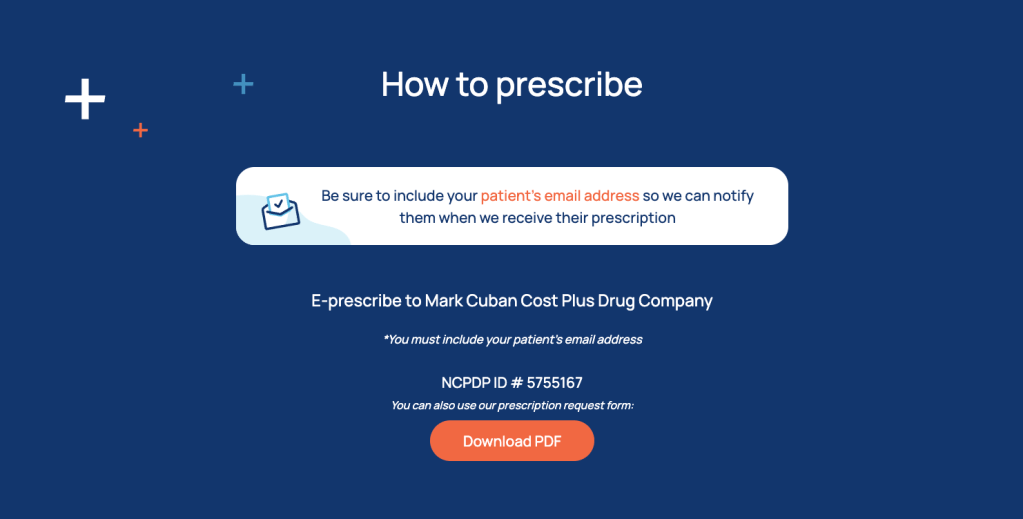
Cost Plus Pharmacy is an online-only mail-order pharmacy owned by that Shark Tank guy Mark Cuban. It shows prices without insurance, so the prices your patient will pay out of pocket. They don’t have every medication, but for the medications they do have, they have pretty good deals.
For example, they are the only place I know of right now that offers generic Entresto tabs for ~$40 for 60 tabs/1 month supply (or ~$20 for a one month supply, if you Rx a higher strength and have your patient cut the tabs in half). Note that these prices are only accurate at the time of this post’s writing, so double check the most current price.
- Go to www.costplusdrugs.com. You can filter by medication type, in this case go to the “High Blood Pressure” section.
- All available anti-HTNsives (including some SPCs) will be listed there, along with their retail price and Cost Plus Pharmacy’s price.
- If you click on a medication, you can toggle around with different doses and quantities to see how prices will change.
- How to prescribe: there’s a whole section called “for providers” on their website. They allow for e-Rxing too. The only thing you have to make sure of is that 1) your patient first creates their own user account with their email address and 2) you put the email address associated with your patient’s account on the prescription.
And that’s it! Have some of your own resources you use? Leave them in the comments!
Until next time –

Great post! For patients without insurance, I also recommend Walmart’s “$4 list”, which offers 30-day supplies of certain medications for as low as $4 or max $24 for 90-day supplies: https://www.walmart.com/cp/4-prescriptions/1078664
If the closest pharmacy is a Walgreens (transportation can be another barrier), this website can search all available drug discount cards to find the one with the best price: https://walgreens.rxsense.com/
LikeLike