Today’s discussion is going to be a little different from my usual teaching spiels and is focused more-so at clinicians – physicians, pharmacists, NPs, PAs, etc – and tips and tools that you can use to help get your patients blood pressures controlled.
It’s nothing new that HTN is extremely prevalent in the USA and one of the factors that heavily contribute to ASCVD morbidity and mortality every year. An estimated ~120 million patients in the US have HTN, and 94.9 million require medication. For those who are on medications, we still see 77.5% of these patients uncontrolled. Let’s say that again:
In patients with HTN in the US on medications, more than 3 out of 4 patients are still uncontrolled and not at goal.
There is clearly a huge unmet need to help these patients get their blood pressure controlled. Besides reducing outcomes and deaths in these patients, as clinicians working with this patient population – you probably are also very familiar with the amount of time, repeat visits, emergent hospitalizations for hypertensive crises these patients require.
Scan the above to get linked right to the latest 2025 Guidelines 😎😎😎😎
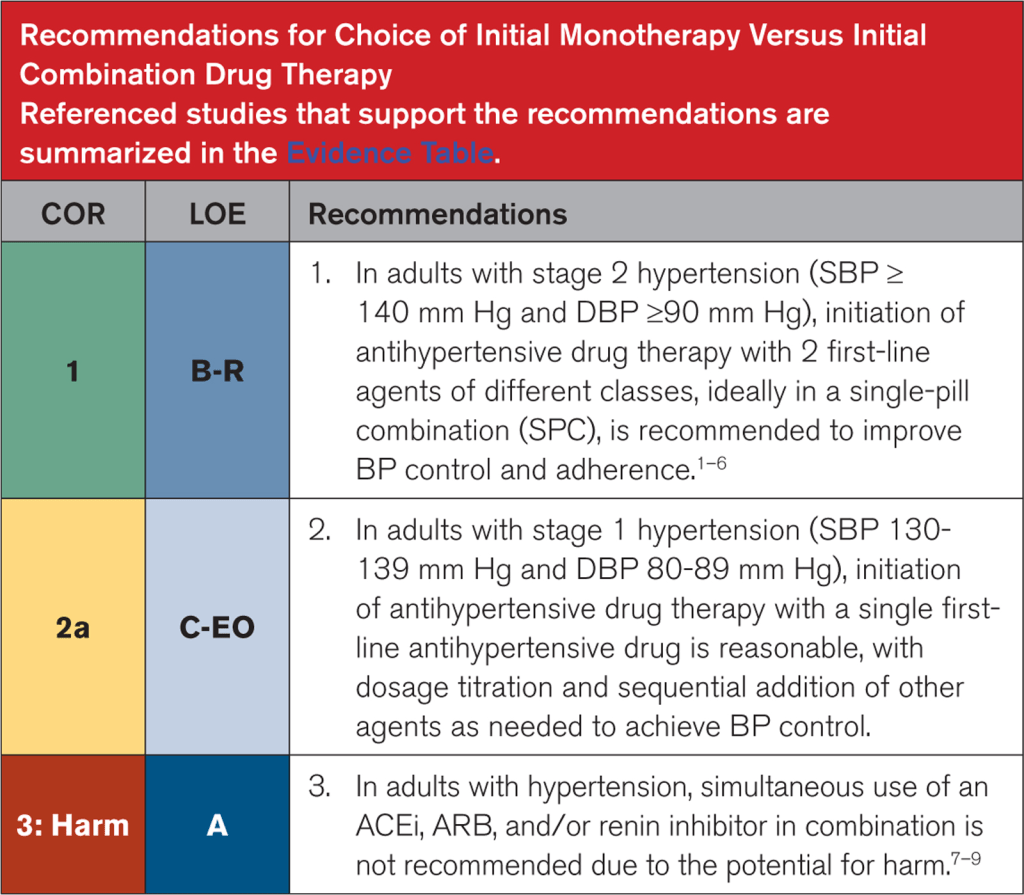
The latest 2025 AHA/ACC/multi-society hypertension guidelines have a new recommendation pushing towards the use of single-pill combination therapy for all patients with stage 2 hypertension.
A big push and change that we see in the latest rendition of the new American hypertension guidelines is this push for the use of single-pill combination (SPC) in patients who present with stage 2 hypertension (defined as SBP ≥140 mm Hg and DBP ≥90 mm Hg – in other words, a big chunk of patients we might see in clinic), ideally with 2 first-line agents of different classes.
Straight from the latest 2025 American Hypertension Guidelines
Now – this idea is not novel – Europe has been recommending this since the 2018 ESC/ESH guidelines (I swear, ESC is always 2 steps ahead of the US…even their guideline figures are cuter).
Investing the time upfront to making sure your patient can get access to their SPCs is time well spent. We’ve all been there – a super uncontrolled hypertensive patient who you’ve ever so slowly gone up on their antihypertensives, but every time they come in, their BP is SBP is in the 160s or worse. SPCs can not only enhance efficacy but also adherence. Investing the time to make sure your patients can get their medications helps prevent back to back clinic visits for sometimes months on end, leaving you more time to focus on other things (all while improving patient outcomes).
The Data: Stepwise Approaches and SPCs
There are no RCTs looking at stepwise approach vs initial combination therapy. However, I think often what a lot of us worry about when adding more than one medication at a time is side effects. We always want to do no harm. How do patients tend to do when starting SPCs?
Well, the data shows us that combining anti-hypertensives with complementary mechanisms not only enhances BP lowering but also might reduce side effects.
Adding a RAS blocker with a thiazide can reduce the incidence of hypo- or hyper-kalemia; combining an ACEi/ARB with a DHP CCB can reduce the incidence and severity of peripheral edema. The latest guidelines say it very well:
“Combination therapy is more effective, efficient, and consistent in lowering BP and improves adherence when using an SPC compared with stepped-care therapy.”
Medications can transform patients lives and prevent terrible outcomes…but only if our patients can get access to these medications. It’s great that the US has finally caught up with recommending these meds, but how does one go about implementing these meds? Some questions that might come up:
What combinations of antihypertensives are even available? Are they generic? How much do they cost? Is there a way to easily find out if we can get these meds at a cheaper cost?
With this new push on this side of the pond, I wanted to share some useful and practical tools that you can utilize to help make sure your patient gets access to these medications. I am not sponsored by any of these resources and am just truly sharing them because I find them helpful. Let’s get into it.
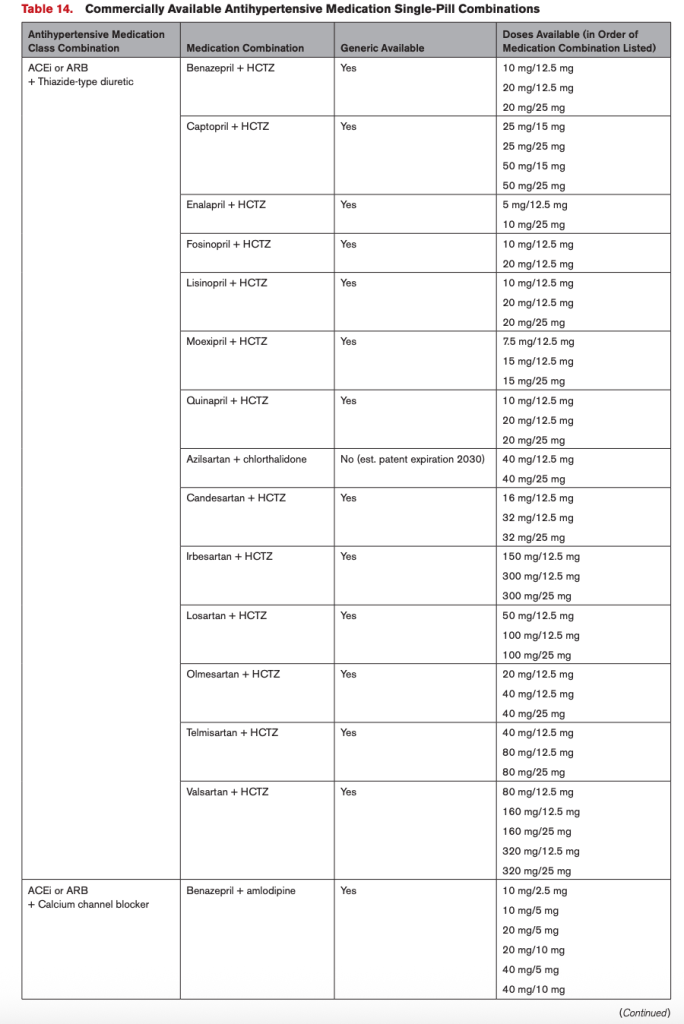
Question #1. I’ve decided I might want to use an SPC in my patient. Now – what the heck do I prescribe? What combinations are even out there?
Cue the updated 2025 AHA/ACC Hypertension Guideline. These people seriously thought it through and made a fantastic resource table. Table 14 of the guidelines have already done that work for US-based providers (see below for a semi-blurry screenshot)
Question 2: Now that I know what SPC’s are available, what about their pricing for my patients?
Pricing is always somewhat annoying to figure out, as every patient has different insurance plans and supplemental plans and blah blah blah. The tools I am going to offer today are independentof insurance (in other words, your patients can get these medications at this rate even if they don’t have insurance). These resources will also provide some references to what the normal out-of-pocket costs would be retail. Unfortunately creating some sort of comprehensive spreadsheet of pricing would not be effective since prices are constantly changing – so the best way to look into prices is looking at pricing in real-time. Below is what I recommend:
Use the GoodRx App.
GoodRx is a free mobile app and website that helps Americans save money by finding them the lowest cash prices on medications. They offer discounted rates on many medications, independent of insurance. If your patient does have insurance, and their copay is lower than GoodRx, then there is no need to use it. GoodRx will not lower your patient’s copay for medications if they are commercially insured. However, if the GoodRx price is lower than your patient’s copay, then they should forgo using their insurance and simply use the GoodRx code to pay an out-of-pocket cash price. Because they are not using their insurance, this will obviously not be applied to their deductible, if they have one.
GoodRx has both a website that you can use, or an app. I really recommend using the app, especially if you actively see patients in clinic since it is way faster and user friendly to use.
Once you download the app, you can make an account as a healthcare provider. There are some handy tools on here:
You can search by your medication. When you search for your medication, it’ll tell you what the retail cost (without coupons), and what the GoodRx price is at different pharmacies, and then in general. You can also “bookmark” your medications. In the example above, I searched for enalapril-HCTZ. It defaults at 10/25 mg 90 tablets and lets me know that retail price is anywhere from $40-90 out of pocket. By using the GoodRx coupon, I know that my patient can get the combo pill from Walmart right now for around $30.
Once you’ve searched a medication, there is a way to easily see other options in that therapeutic class. In the example above, I initially searched for enalapril-HCTZ. You can then look at other meds in the ACEi/thiazide class.
Once you are on a particular medication, you can play with some options like changing the dose or quantity of the medication. For example, if you need 180 tablets, you can input this to see what the updated price will be.
How it works: When you click on the price, you will get a screen (see above) with codes for the pharmacy team to input at the pharmacy. Your patient should present this information to the pharmacy staff when they go to pick up their prescription. You can also share this information quickly with your patient or others by selecting the “text” or “email” options.
If you go to your home page, you can see all of your bookmarked medications. I’d recommend adding the SPCs to your bookmarks so you can quickly see their prices while prescribing, instead of having to type in each separate medication every time.
2. Check out Cost Plus Pharmacy
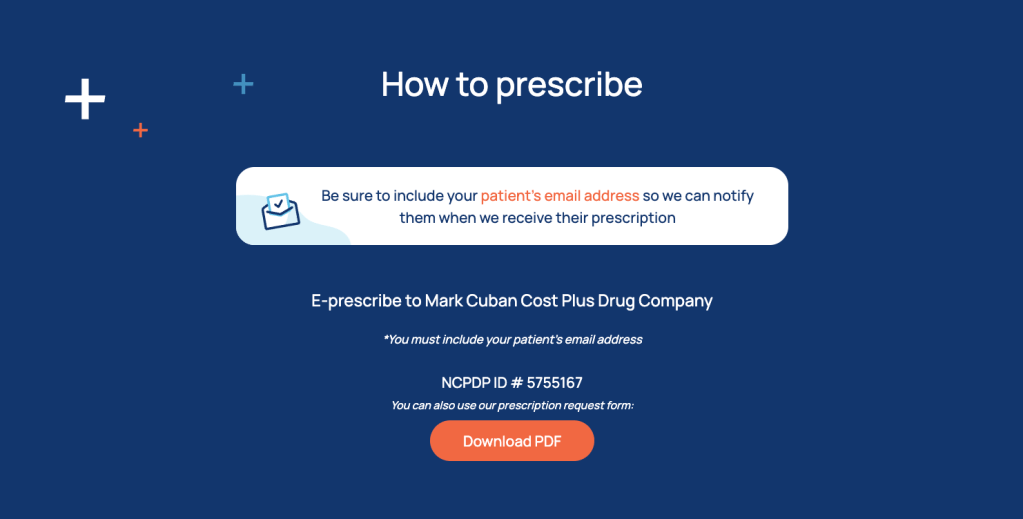
Cost Plus Pharmacy is an online-only mail-order pharmacy owned by that Shark Tank guy Mark Cuban. It shows prices without insurance, so the prices your patient will pay out of pocket. They don’t have every medication, but for the medications they do have, they have pretty good deals.
For example, they are the only place I know of right now that offers generic Entresto tabs for ~$40 for 60 tabs/1 month supply (or ~$20 for a one month supply, if you Rx a higher strength and have your patient cut the tabs in half). Note that these prices are only accurate at the time of this post’s writing, so double check the most current price.
All available anti-HTNsives (including some SPCs) will be listed there, along with their retail price and Cost Plus Pharmacy’s price.
If you click on a medication, you can toggle around with different doses and quantities to see how prices will change.
How to prescribe: there’s a whole section called “for providers” on their website. They allow for e-Rxing too. The only thing you have to make sure of is that 1) your patient first creates their own user account with their email address and 2) you put the email address associated with your patient’s account on the prescription.
And that’s it! Have some of your own resources you use? Leave them in the comments!
Hey everyone! Today we are going to discuss what therapies we have to get our post TAVR patients on, and why. ICYMI, I would recommend reading Part 1 first.
I’m back to discuss antithrombotic management post TAVR (woohooooo)
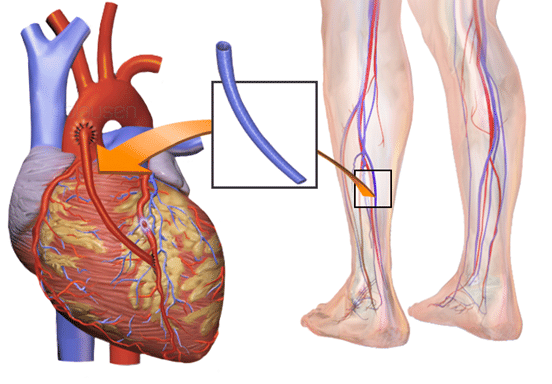
We already discussed what TAVRs are – essentially a less-invasive, catheter-based version of replacing a patient’s aortic valve. Instead of having to undergo open heart surgery, cracking the chest open, going on bypass, etc – you just need to make a little incision in a large artery and thread a catheter through and deploy the valve that way.
To get a good idea of what this procedure looks like, I would recommend watching this video. Also special shoutout to UC Davis where I did my residency (Dr. Southard was a fantastic teacher on rounds).
When I think of TAVRs, I almost think about them as a valve version of a cardiac stent – after all, coronary artery stenting was really the basis behind where the TAVR inventor got his ideas from (he even called the TAVR valve a “stent-valve”).
Now, let’s think back to the TAVR procedure and some complications that can happen as a result. We already talked about the main procedure-related complications – mostly access site (wherever that nick to access the artery was made) bleeding and strokes that form as a result of some of that old calcified valve flicking off, or a clot forming during the procedure.
Similar to how we approach surgical valves (or really any foreign object exposed to our bloodstream) something that has to be on the forefront of our minds when thinking about post-TAVR management is reducing the likelihood of valve thrombosis and systemic embolisms (check out clot formation 101 if you need an overview about why clots form).
When we introduce that new valve in the area around your old, crusty aortic valve, squish that old valve out of the way, and leave this new valve in its place, we are essentially telling our body’s coagulation system to wake up and get going.
No one: The valve to the coagulation cascade:
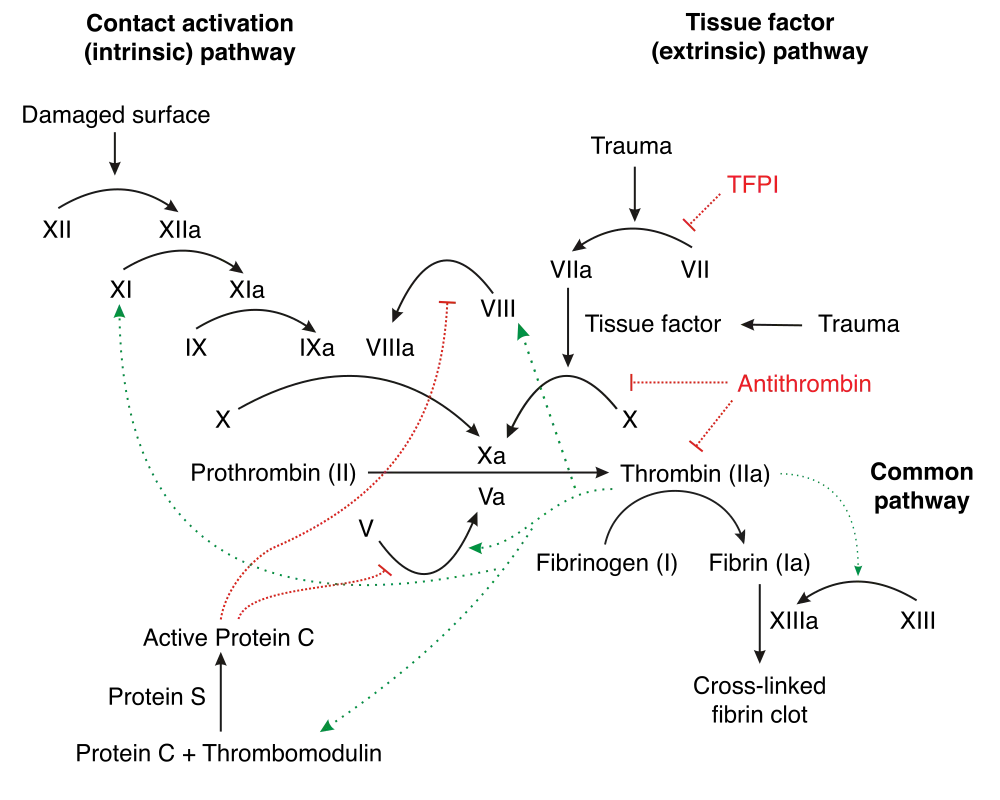
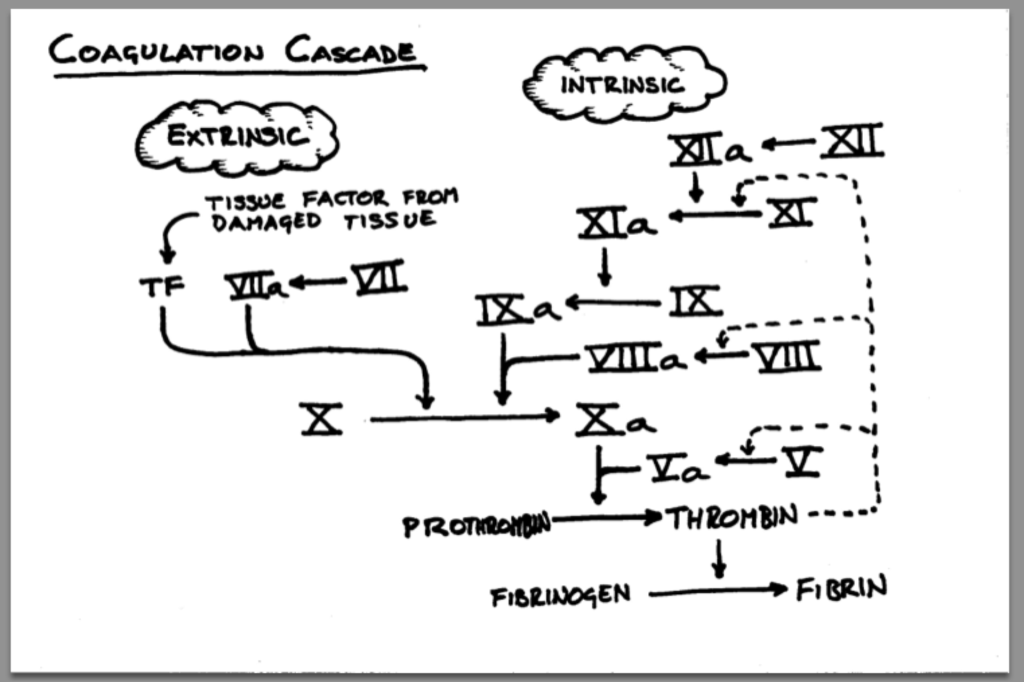
The tissuedamage that is caused by the manual crushing of the old aortic valve exposes tissue factor (TF) to the bloodstream, activating the extrinsic coagulation cascade. And that brand new shiny tissue valve is also a foreign surface in the bloodstream which activates the intrinsic coagulation cascade.
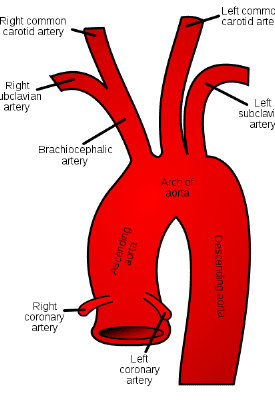
Just like we do for any valve replacement or coronary artery stenting, we have to worry about ameliorating these risks and protecting our patient from forming a clot on or near this new valve surface. If clots form here, the risk of a stroke is very high...all that clot needs to is flick off that aortic valve and take a 1-way trip up the aorta and into the brain (check out the coronary anatomy post if you need a refresh on the anatomy of the cardiovascular system and why a clot on the aortic valve would likely cause a stroke).
When talking about what kind of antithrombotic therapy we need in these patients, I’m going to chat a little bit about
what we used to do, and
how the landscape of antithrombotic management has changed in recent years.
The original TAVR antithrombotic regimen of choice
When TAVRs were first designed, created and used in the early 2000s, because they were intellectually modeled after coronary artery stents, their antithrombotic regimen was also modeled after what we do in coronary artery stenting: DAPT.
Coronary Artery Stenting and TAVR pharmacotherapy management in the early 2000s:
At the time, taking a page out of what we did for coronary stents, the practice was to use clopidogrel + ASA for around 3-6 months, followed by aspirin monotherapy.
Early post-TAVR management involved DAPT (clopidogrel + ASA) for 3-6 months followed by aspirin monotherapy.
The reasons behind this were likely multifactorial, the strongest being that TAVR was somewhat analogous to PCI. Because TAVR was modeled after coronary artery stents, the antiplatelet therapy regimen was largely borrowed from the same protocols that were used in PCI. Because we used DAPT post PCI to prevent thrombosis, it was then assumed that this would be the best bet for managing our post-TAVR patients.
The cutoff of 3 to 6 months was employed because studies have really shown that 3-6 months is the amount of time it takes post-implantation for the valve to start endothelizing, dramatically reducing the risk of thrombosis (after all – if there is no metal/foreign object exposed to the bloodstream, the risk of thrombosis really goes away).
Because TAVR was also a fairly new procedure, there was a lot of early concerns about the possibility of thrombosis, specifically valve thrombosis, strokes/TIA, or even coronary embolization. The interesting thing is we really didn’t have any data to back up this strategy – in other words, DAPT was kinda just what was chosen from the get-go, and in the absence of evidence saying the contrary, this more aggressive platelet inhibition strategy was employed.
All of us in healthcare doing the best we can with what we know everyday:
As an aside – learning about the way we figured out things in medicine was always very interesting to me. When I was younger there was this thought that we just “know” what to do in medicine. But the more you learn about medicine, the more you learn that we are just making it up the best we can as we go along with the best data we have at the time.
When people start questioning the “status quo”…
Although the use of DAPT was standardized for our TAVR patients, there were some people questioning the need for this aggressive platelet inhibition pretty early on.
Do we even need DAPT for these patients?
Why the questioning? It’s most likely due to a few reasons.
1) we know that in surgicalbioprosthetic aortic valve replacements, aspirin alone is generally enough and our standard of care to manage these patients and to protect them from thrombotic complications. One could argue that TAVRs may cause less thrombotic complications than SAVRs since they are greatly less invasive and do not involve the cutting out the old valve.
2) at the end of the day, the environment around the aortic valve is greatly different than the environment around our coronary artery stents. The coronary arteries are waaaay tinier/narrower, have slower flow, and lower pressures. In contrast, the area around the aortic valve is high pressure, high flow, and has a fairly wide circumference. All of these factors promote the idea that coronary arteries are likely far more likely to develop a clot when a stent is deployed there, versus the area around a TAVR valve.
3) Safety. We also know that SAPT is also overall safer in terms of bleeding versus DAPT. There could be a potential benefit from de-escalating therapy and reducing the risk of harm in terms of bleeding events.
Ussia et al. challenge the norm
In 2011, Ussia et al. decided to put this idea into practice. They conducted a small (n~80) randomized, single-center, prospective pilot study that compared DAPT (clopidogrel + ASA) for 3 months versus ASA 100 mg PO QD (the 100 mg dose was used over the 81 mg dose likely because the 100 mg dose is what was available in the country where this study was conducted).
The primary endpoint looked at all the important stuff – major adverse cardiac and cerebrovascular events – and maybe not surprisingly to some, they found that the cumulative incidence of their primary endpoint at both 30 days and at 6 months (the end of that most thrombotic time period post implantation) was not statistically different between groups.
Though promising, Ussia et al recognized that these results must be confirmed by larger RCTs, but they largely paved the way for this question to continue to be studied.
Others follow suit and lay the groundwork for something big…
Over the next couple of years, a variety of trials, studies and meta-analyses are published looking at this same question. In 2014, we had the SAT-TAVI trial by Stabile et al investigate this question again- this group was somewhat larger (n~120). Once again, they did not find differences in terms of thrombotic outcomes.
In 2017, the ARTE trial was published by Rodes-Cabau et al and was a prospective, randomized, open label trial of ~220 patients looking at DAPT vs ASA and showed that SAPT tended to reduce the occurrence of major adverse events following TAVR, reduced the risk for major or life threatening events, without an increased risk of MI or stroke.
These results were repeated in 2019; a meta-analysis by Kuno et al. investigated a slew of different antithrombotic therapies post TAVR. With a robust total population of over 20,000 patients, they found that SAPT (ASA alone) had a significantly lower rate of bleeding versus DAPT, without any differences in stroke. In other words, this meta-analysis hinted that choosing ASA upfront not only reduced the risk of bleeding, but didn’t have any trade-off in the incidence of stroke and still offered enough thrombotic protection for these patients.
These important studies and trials over the span of a decade paved the way for something bigger to confirm their findings and change practice….
The POPular-TAVI trials
In 2020, we finally had a large RCT come out confirming the results of all the studies previously. The PoPular-TAVI trials can be a little confusing, since there are 2 different papers published based on what cohort they studied. One branch (cohort A) of the study looked at your normal run-of-the-mill patients post TAVR and compared aspirin with or without clopidogrel. We will talk about the other cohort a little later (I’m sure the suspense is killing you).
The moment a lot of us TAVR nerds had been waiting for…The POPular TAVI trial (Cohort A)
This arm of the POPular TAVI trial was an RCT in patients undergoing TAVR who did not have an indication for anticoagulation (in other words, they weren’t already on OAC for a hx of VTE, or AFib, let’s say). Over 600 patients were randomized to either receive aspirin alone or aspirin + clopidogrel for 3 months. The primary outcomes looked at bleeding and non procedure related bleeding over a period of 12 months. The secondary outcomes look at a composite of death from CV causes, non-procedure related bleeding, stroke or MI (aka ischemic + bleeding complications together) and a composite of death from CV causes, ischemic stroke or MI at 1 year (aka ischemic outcomes alone). The results indicated that the incidence of bleeding and composite of bleeding or thromboembolic events were significantly less with ASA versus DAPT for 3 months. When looking at thromboembolic events alone at 1 year, ASA reached non-inferiority but not superiority (which is kinda expected).
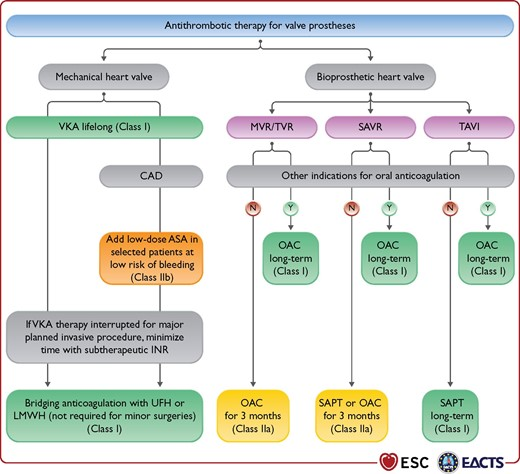
Though the POPular-TAVI trial greatly impacted clinical practice, this rec is not included in the latest valvular US guidelines because POPular-TAVI was unfortunately not published in time to be considered for inclusion.
However, because the European Guidelines (ESC) were published a year later, the recommendation to use SAPT after TAVR was incorporated.
Long story short, in most patients post-TAVR who don’t have a compelling indication for OAC, SAPT is now really the standard of care.
Why do we even do antiplatelet therapy in these patients post TAVR, rather than oral anticoagulation?
Like I said above, we did DAPT from the start with little to no evidence, and so at some point or another the question came up whether or not OAC would be a better strategy in these patients. This is what the GALILEO trial looked at, and found that patients who received rivaroxaban 10 mg PO QD had a higher risk of deathor thromboembolic complications as well as a higher risk of bleeding than an antiplatelet-based strategy.
IYKYK
In other words – OAC in patients that don’t have an indication for OAC? Not good.
Galileo
What about those with a pre-existing indication for OAC?
Now that we know that SAPT is the best, evidence based treatment of choice post TAVR in most patients, I’m sureeeee you are thinking – what do we do for patients that need to be on oral anticoagulation for another reason (e.g. AFib, VTE)? Do we put these patients on OAC + SAPT? Do we do OAC alone?
Luckily for you, this is where cohort B of the POPular-TAVI trial came in.
The second cohort I promised you!
This trial sought to answer that exact question. The investigators conducted an RCT of patients undergoing TAVR who had a pre-existing indication for OAC. Patients were then randomized to either receive clopidogrel (aka OAC + clopidogrel) or no clopidogrel (aka OAC) for 3 months. The trial found that serious bleeding was higher with OAC + clopidogrel versus OAC alone. OAC alone was also non-inferior to OAC + clopidogrel, though the non-inferiority margin was big.
The POPular-TAVI cohort B trial showed that OAC alone, rather than OAC + clopidogrel should be used post-TAVR in patients with an indication for OAC.
This trial then became the basis for ESC’s other statement recommending OAC (rather than OAC + clopidogrel) in patients post TAVR with a pre-existing indication for OAC.
Now if you’re me, I know what you might be thinking – it’s kinda a bummer that this trial looked at OAC + clopidogrel, and not OAC + ASA. Afterall, it’s aspirin, not clopidogrel that we put on for the other patients post TAVR.
The AVATAR trial sought to clarify this further.🎉🎉🎉
But although to my knowledge, although completed, the results haven’t been published anywhere or presented at any conference.
Womp, womp. Hopefully those results will be posted sooner than later.
And that, my friends is the antithrombotic management of patients post-TAVR. Most patients will get SAPT with aspirin. In those with another indication for OAC, most patients will get OAC alone.
OK, one more thing but this is just extraneous info, more related to drug literature analysis (so totally skip if you want)!
Whenever you read a trial, always make sure to keep a close eye on how trials are defining their endpoints. Afterall, I always say a trial can basically do or say whatever they want as long as they define what they mean.
A good example of the quirks behind how trials can define their endpoints would be how they defined bleeding in the POPular-TAVI trials. Now, keep in mind, the majority of bleeding that we worry about post TAVR is access site bleeding, or the place where we inserted the catheter to conduct the procedure.
However, the investigators of this trial defined their procedure-related bleeding as any BARC type 4 severe bleeding.
BARC is one of our commonly used methods to characterize bleeding in trials – other commonly used ones are GUSTO, TIMI, and ISTH.
If you actually look at BARC type 4 bleeding, you will see that this bleeding is also called “coronary artery bypass grafting-related bleeding“, aka the type of bleeding you would see after an open heart surgery.
Bleeding under this category includes “perioperative intracranial bleeding within 48 hours; reoperation after closure of sternotomy for the purpose of controlling bleeding; transfusion of 5 U of whole blood or packed red blood cells within a 48-hour period; chest tube output 2 L within a 24-hour period.”
Considering TAVR patients don’t have 1) a sternotomy to begin with, or 2) chest tubes, this type of bleeding may not have been the best way to categorize true bleeding for these patients.
None of these capture your typical TAVR-related bleeding – and so – for the purposes of the POPular-TAVI trials, access site bleeding was considered non-procedural bleeding.
At the end of the day, the POPular TAVI trials still were landmark trials, but while we were talking about them, I thought it might be a good little drug lit lesson to throw in there. Always look at how trials define their endpoints. A lot of times this info might be hidden in the supplemental, but it may or may not change how you view the clinical relevance of the results.
Hi guys! It’s been a while. Have been busy with work and life, and ya know, casually had a baby, who has since turned 1! Here’s my little lady on Halloween (she was Dumbo).
Anyway, today we are going to talk Transcatheter Aortic Valve Replacements, also known as TAVRs (pronounced TAHVER). TAVRs are one of the things that I geek out to my learners about, since they are truly an example of modern technology totally changing the landscape of medical care.
Just 1 or 2 decades ago, the only way we could replace a patient’s aortic valve was to cut them open, crack open their ribs, put ’em on bypass, and do a whole open heart cardiothoracic surgery. If you remember from our earlier talks on valvular disease, this posed quite a problem – especially since a good chunk of our patients who would need this operation tended to be old and at higher risk for complications with such a large surgery. But – then again – if we didn’t do a surgery, these patients would either develop heart failure and/or their HF would progress. It was kinda like a whole “between a rock and hard place” kind of situation.
Let’s talk a little history of how these modern marvels came into being.
History of TAVRs – a story that should remind you to never give up
The year was 1989. Big hair was slowly getting smaller as the 90s approached and a Danish cardiologist in his 30s named Dr. Henning Rud Andersen was attending an interventional conference in the US where the developer of the balloon-expandable stent was talking (but also isn’t it crazy that even cardiac stents are so fairly new in the grand scheme of medicine?). Coronary artery stents were all the rage and all of a sudden it hit Andersen – if we can deploy a stent in the coronary artery with a balloon, why can’t we use a balloon and build an expandable heart valve with a metal frame?
When he came back to Denmark, he shared his idea with some colleagues and professors, many were skeptical and called him crazy. But Anderson took a page out of Taylor Swift’s book and shook off all his haters and continued on his idea by himself, without any funding or industry support.
Andersen to all his haters
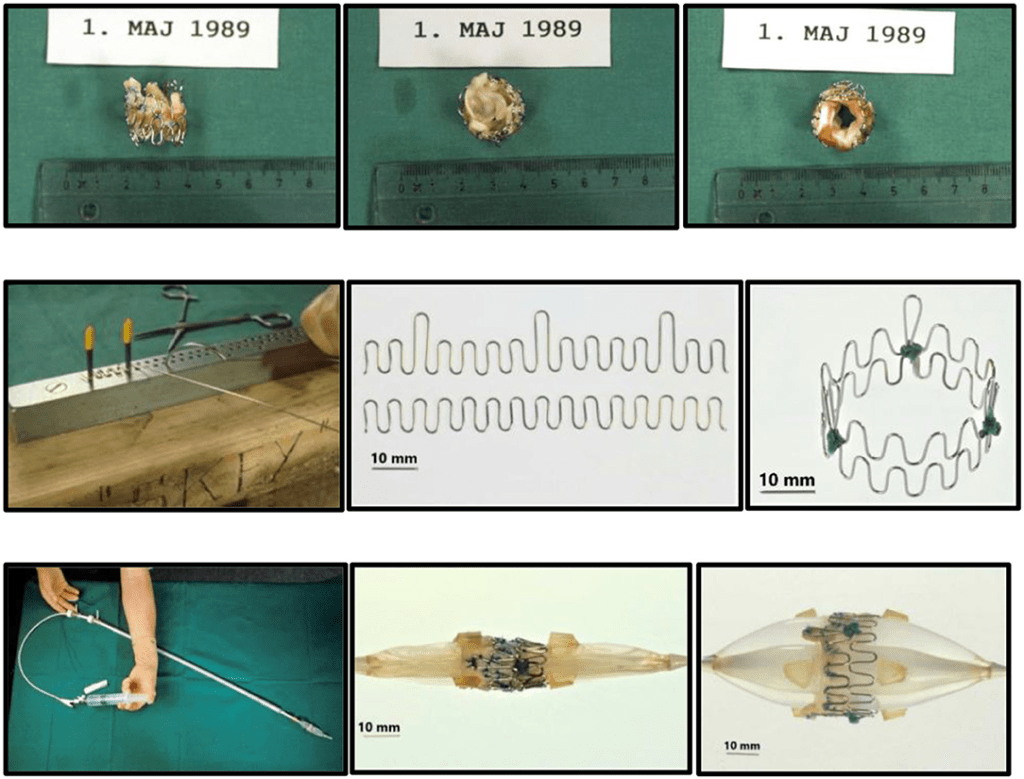
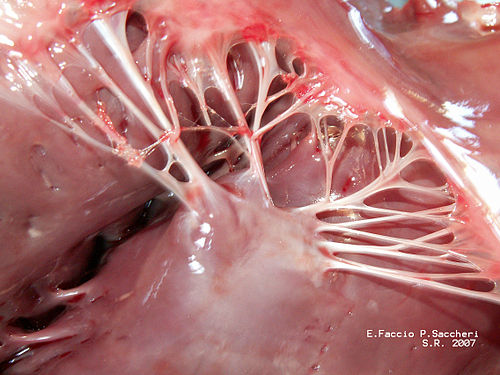
This guy quite literally MacGyvered a valve prototype – he went to local hardware stores and bought steel and iron wires to build his struts for his valve and soldered his first prototype together. It took a lot of trial and error – too thick, and the wires were too stiff to get good dilation by just a balloon, too thin and the wires failed to maintain structural integrity. Per Andersen himself everything was done by eye aka evaluation was done by “simple visual observation and gentle finger compression”. He also went to local slaughterhouses and bought pig hearts, carefully cut out the aortic valves, and mounted them in the stent. He had to re-use balloon catheters after being used in patients, which often did not fit and were too small for the aortic valve size of pigs, where he would refine the technique in (for reference, adult aortic annuli are like ~6 mm; pig’s are like 13mm!)
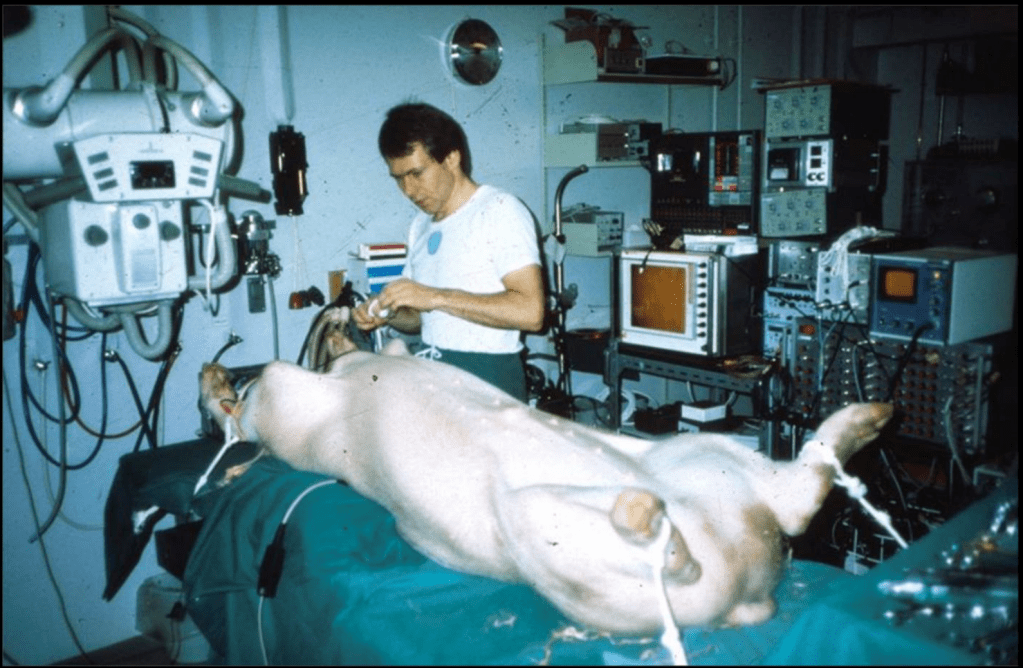
Just months after his initial idea, Andersen did his first-in-animal implantation in May of 1989 on an adult kg pig and it was a success. The other crazy thing was that in pigs, the femoral artery was too small to access (e.g. only 3-4 mm wide) and so he obtained access to the aortic valve by performing abdominal surgery and going through the ABDOMINAL AORTA. woof – so much for “minimally invasive”. Not surprisingly, in his initial days, sometimes the pigs would die even before implantation due to the extensive abdominal surgery.
Andersen’s First-in-Pig procedure, May 1989Like I said – accessing the abdominal aorta for access was quite a challenge. So much for minimally invasive 😉
Sometimes the balloons ruptured before fully inflated because they were makeshift quality . Sometimes he would implant them and the valve itself would block area of the aorta where the pig’s coronary arteries branched off (aka the coronary ostia). Sometimes the valve dislodged and broke off because the size was smaller than that of the pig’s aortic annulus (width where the aortic valve sits). Sometimes the whole thing would be pushed downstream and end up in the ascending aorta with blood flow. As Andersen said years later, he learned that “one size of pig does not fit all secondhand balloon catheters!”. One poor medical student even implanted the valve upside down (Andersen still mentions this years later – can you imagine being that poor unnamed med student who made a mistake and are still low key living in shame all these years later when he/she sees articles about it!?).
The coronary ostia
Another issue was that it was really hard to precisely implant/expand a valve in such a wild fast-moving area. Think about it – the aortic valve sits right where that left ventricle is squeezing out blood super, super strongly. To fix this issue in the early days, Andersen literally temporarily stopped all blood flow by inflating another balloon and placing it in the common pulmonary trunk. WILD.
But…more challenges.
In 1990, Andersen and his team submitted an abstract in hopes to present his poster on his initial work….and it was rejected.
That same year, he submitted a manuscript to a journal for publication for this ground-breaking work (submitted to JACC) – and…was rejected.
Then they tried again, and submitted to Circulation, another journal – who quite literally responded with “I do not see any possible use of it in patients with calcified aortic stenosis” (bet that reviewer is eating their words now). Suffice to say, their publication was once again rejected.
Andersen low-key kept his rejection letters and I AM SO HERE FOR THIS LEVEL OF PETTY.
They finally submitted to a journal with a “extremely low impact factor” and were accepted; another paper was accepted in another little-known journal.
With these publications, Andersen finally got accepted to present at ESC, but only as a poster presentation. Needless to say, his team was bummed. Per Andersen it seemed that they “could not be published in major prestigious journals with high impact factors ort presented as oral presentations at international conference”.
Anderson at ESC 1992, presenting his work among a billion other poster presenters.
Eventually, some other cardiologists and scientists heard of his work, and started replicating it in other animals like dogs, and eventually it was attempted on patients who were so high risk for surgery, no surgeon would touch them.
Fast forward through many decades of persevering in the face of opposition, likely imposter syndrome, and not listening to all the haters and….
Started from the bottom, now we’re here
The year was 2011. TAVR had since become more accepted, with the first in human completed in 2002, and its popularity slowly growing.
Andersen’s father is found to have severe, symptomatic aortic stenosis at the age of 86. Too old and frail for cardiothoracic surgery, his father QUITE LITERALLY UNDERWENT TAVR which saved his life.
Andersen and dad s/p TAVR implantation
Let me say that again.
Andersen’s work from over 20 years earlier saved his father’s life 22 years later. The procedure was a huge success and his father was walking the same day as the procedure and home a few days later. He lived for another 8 years without cardiac issues and died at the ripe age of 95. If Andersen had given up when times got tough years earlier, his father might have arguably died at the time.
The most iconic story in all of cardiology.
This story lends credence to the idea of never giving up, silencing out your haters, and never letting imposter syndrome get to you. Let that sink in.
TAVR today
TAVR today is getting more and more popular, and is frequently performed. Luckily for us, the procedure is now minimally invasive, a far cry from the initial days of abdominal aortic access with Andersen’s pig friends.
Access is usually accomplished through the femoral artery but other accesses such as subclavian is possible. The procedure is done by an interventional cardiologist (same people who put in stents but usually with some additional valve training) in the cath lab and is done percutaneously with a catheter.
The video above is a nice visual to show how implantation is done. The catheter in inserted in one of those large arteries, and goes against blood flow up, up the aorta, through the descending aorta until it reaches the site where the aorta valve sits. This is where deployment happens.
Source: MyHeart.net
Thankfully for us, we don’t actually do any specific occlusion of arteries or veins to get blood flow cessation. However, it still is important to get minimal cardiac output as the interventionalist places the valve, since unlike some other procedures (like the MitraClip), this is a one shot thing. Once placed, you can’t reposition the valve and try again. Which means if it is misplaced, oftentimes the baton will be passed to the cardiothoracic surgeon to go in and fix the issue physically – which means an open heart surgery.
To help decrease cardiac output, we induce rapid ventricular pacing during implantation. Right before implantation, a pacing wire placed in the left ventricle will be turned on, and basically induce almost like a ventricular fibrillation vibe in that LV. In other words, we can make the LV stop contracting hard and reduce cardiac output for a few seconds as that valve in placed so it can be placed precisely.
Check ut that LV quivering! Source: MyHeart.net
Complications
Although TAVR is much better tolerated than an open-heart cardiothoracic surgery, it carries risks just like anything else. Let’s think through some of them together.
The first maybe more obvious thing has to do with the access itself. You’re entering a major artery, which is a high pressure system. While this is done pretty routinely these days, you still carry a risk of bleeding at the access site (albeit much less than what we see with open heart surgery). Procedure site bleeding, along with bleeding after the procedure due to the pharmacotherapy you have to take with it (we will talk about that next time) is really one of the biggest risks of TAVR. Patients also need systemic anticoagulation during the procedure so no clot forms on, or flecks off of the catheter. Other things that come with catheterization can also happen like risk of infection (especially when femoral access is obtained – we tend to have a lot of nastier bugs “down there” in that area) and rarely risks of things going awry with the procedure itself like misplacement of the valve or the catheter wire perforating something.
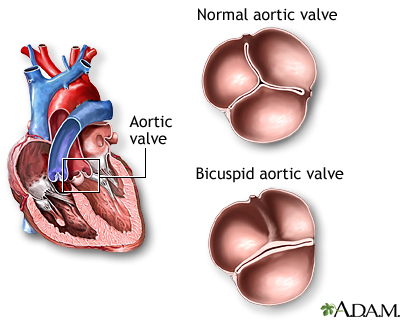
There is also a theoretical risk of occluding the coronary arteries, though this is very rare since the team carefully accounts for their anatomy (which is occasionally why some patients may not be good candidates for TAVR).
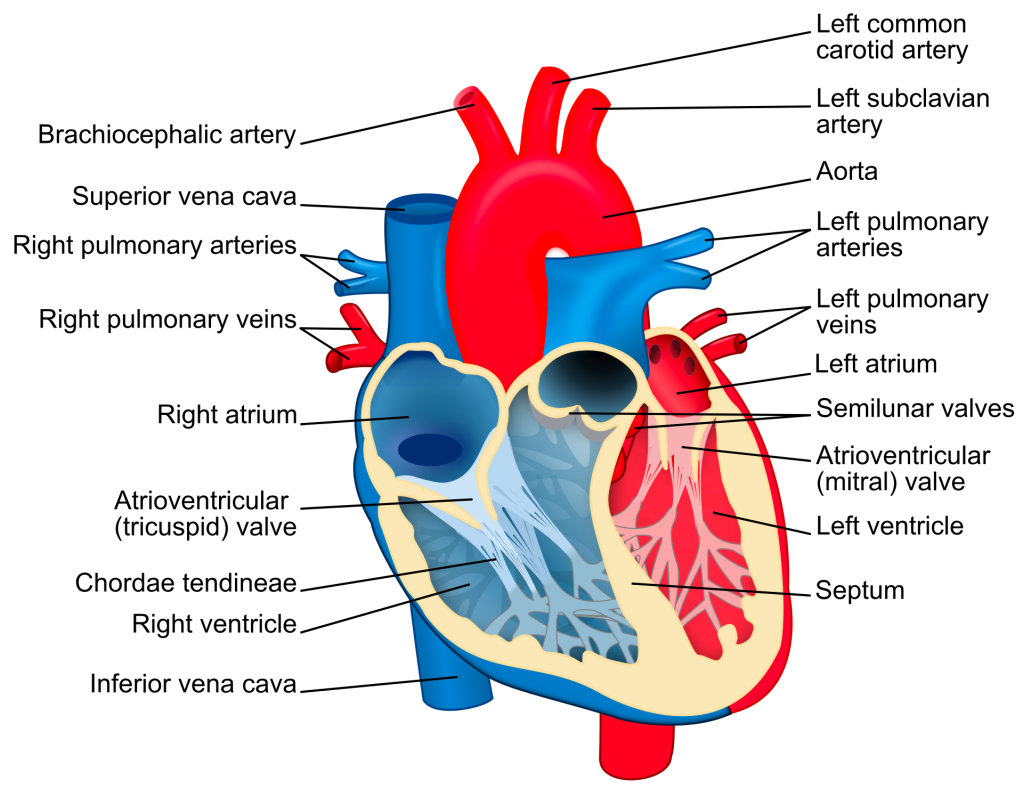
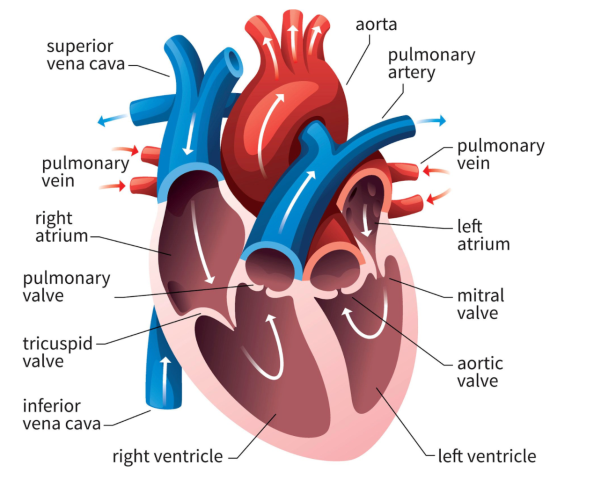
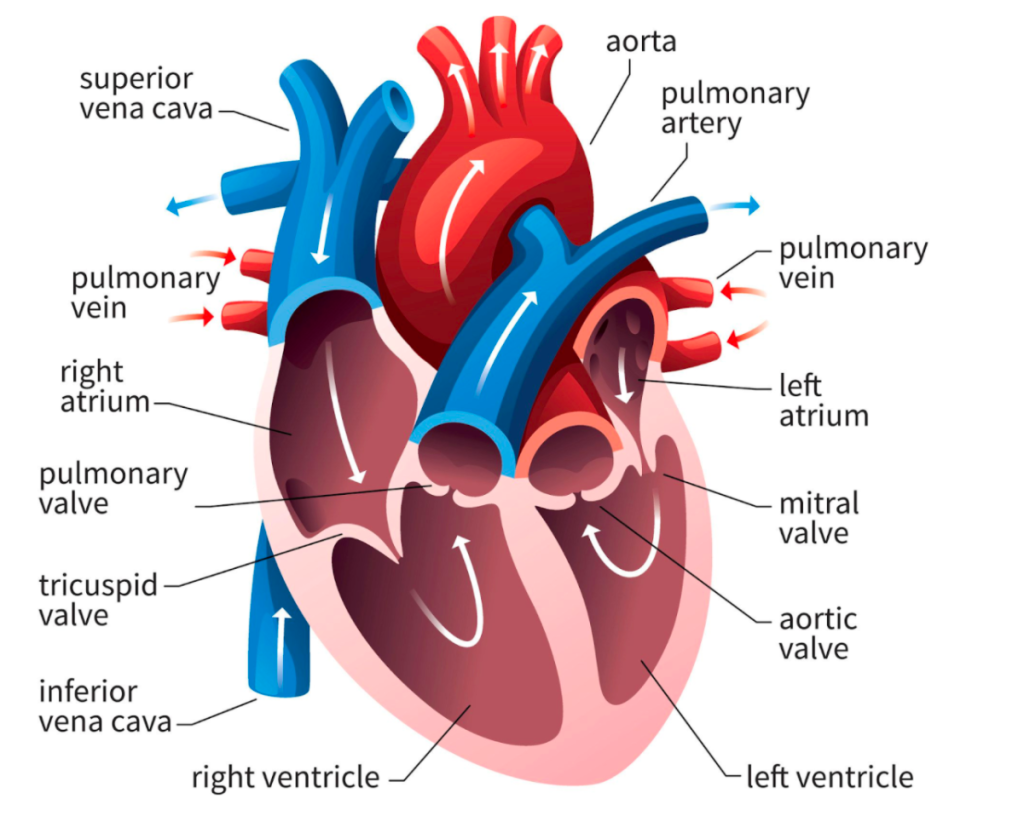
The aortic valve sits right at the bottom of that diagram, and as you can see the coronary arteries branch out nearby. Souce: ThoughtCo
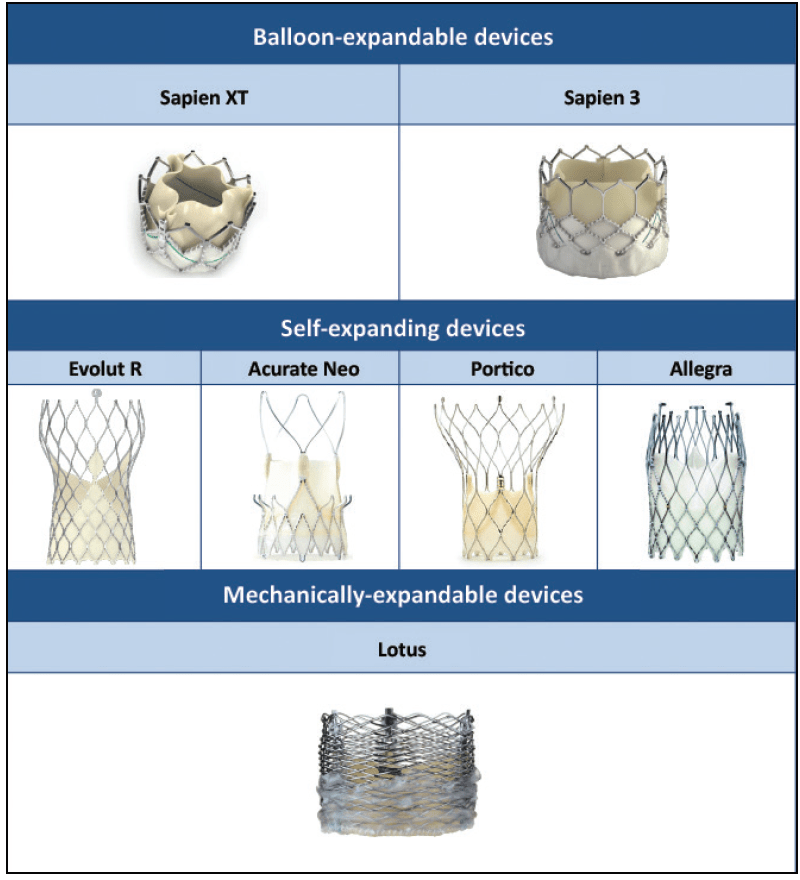
We also have quite a bunch of types of valves to now choose for to do this procedure with. Some are much shorter, meaning they may not interfere with the coronary arteries; others that tend to be longer, purposefully try to make their mechanical strut pattern wide so that, if needed, coronary access may still be possible in the future if needed.
Source: Cardiac Interventions Today
The team will often do a coronary artery catheterization to check for any significant coronary artery disease in their initial evaluation for TAVR since once a TAVR is deployed, coronary access may be harder since one of the metal struts may make it hard to maneuver into that area. Better to clear a patient prior or perform necessary PCIs prior to make sure their coronaries won’t be a problem in the future once they’ve gotten their valve.
Besides bleeding, another complication of TAVR is valve thrombosis. Afterall, you are putting in this foreign tissue with metal strut object into your bloodstream, and we all know the coag cascade loves a foreign object to get itself worked up and activated. The risk is fairly low – compared with, let’s say a fresh coronary artery stent – but we will discuss this when we discuss medications in our next post.
Source: Classnotes123
Another more major complication of TAVR is stroke. If you noticed, not once in this whole post have I said we actually remove the pre-existing crusty valve that a patient had in there. When TAVRs are done, that old valve is simply pushed out of the way with the deployment of our new valve. As this valve is pushed out of the way and crumpled, it is very possible that flecks of the calcified tissue can break off – and once off, these pieces have a one-stop shot straight up to the brain and can cause an ischemic stroke, since the major arteries carrying blood to the brain are located soon after in the aorta.
To prevent this from happening, these fancy “embolic protection devices” have been created. These are basically fancy nets that filter and protect the major vessels that go to the brain and these are deployed during the TAVR procedure and then taken out .
Who wants to go fishing? Source: TCTMD
Source: TCTMD.com
From the interventionalists I’ve talked to, it is not uncommon at all to find some crud in these nets at the end of most TAVR procedures. Exhibits A and B below:
The stuff of nightmares.
Crazy how something so little can be so devastating. Source: DAIC
Despite these devices, strokes can still happen after these devices are removed, especially in those early days post TAVR implantation. Or, besides calcified material, it’s also possible that some clot can form as a result of the tissue damage in that area, and a clot can flick off and embolize and cause strokes. Besides strokes, technically any of those evil flecks above can cause any arterial embolism if blood flow carries them past those vessels that carry blood to the brain and further down the aorta.
Hope you enjoyed today’s TAVR background. It’s one of my favorite stories to tell, especially to learners. Next post we will focus on pharmacotherapy and what these patients need post-TAVR, including a little history of how these meds have evolved over time. Thanks for tuning in!
Now that we’ve solidified the basics of valves – why we have ’em, how they work, all the squirrely stuff that can go wrong with them – let’s talk about how we actually can treat these patients.
We’re going to be reviewing treatment of these conditions prior to surgery/replacement and then review what therapies these patients should start on after they get their bright new shiny valves.
Now, the therapies below for our “pre” valve replacements are not a fix – they are merely bandages while you figure out when your patient can go for replacements.
This talk today will only focus on surgical valve replacement – part 3 will focus on other methods of valve replacement (e.g. TAVRs).
Understanding the pathophys of what’s going on with these valves will be very very important! So if you haven’t plz read part 1 first because I will only be doing a basic recap here.
“Treating” Valvular Disease Prior to Surgery
Aortic Stenosis
OK – so in aortic stenosis (AS), we have this really crusty, calcified, narrowed aortic valve.
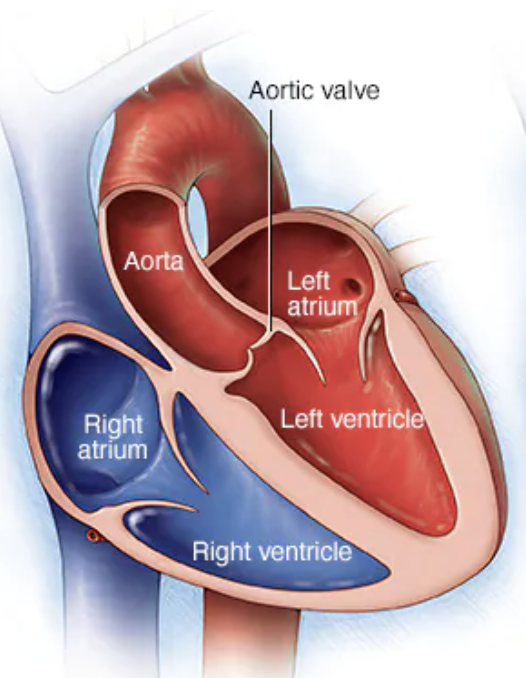
Keep in mind that the aortic valve is our gateway between the left ventricle and the aorta – it’s the last stop in the heart before blood is shot out to the rest of the body.
aortic stenosis IRL. Woof.
Managing blood pressure in these patients is going to be key prior to them getting their valves replaced.
Afterall, put yourself in the shoes of your left ventricle.
In aortic stenosis, that LV is already struggling to get blood out and keep forward flow because it is quite literally trying to push all this blood through a teeny tiny cocktail straw (think about how your cheeks feel after blowing through a slurpee straw versus a cocktail straw for a long period of time). It’s going to create chronic high pressures in the LV (and thus over time hypertrophy and heart failure).
The last thing we want to do to that poor LV is make it even harder to get forward flow by having your patient run grossly hypertensive.
With high blood pressures, that huge afterload that the LV already has to pump against is just going to get even worse. The rule of thumb in these patients is that we’d love to avoid gross hypertension because of this.
But….it gets complicated *bum bum bum*. Let’s talk about why.
Quiz question/check your memory: What are the two determinants of blood pressure in the body? AKA what is the formula for blood pressure?
*insert brain storming here*
If you don’t remember – totally cool – but I’d recommend a refresher (check out the hemodynamics OG post).
Blood pressure is determined by both 1) blood volume and 2) squeeze of vessels.
Our blood volume is represented as cardiac output (CO) – aka the amount of blood your body gets per unit of time. The squeeze of vessels is known as systemic vascular resistance, or SVR.
Let’s say you gave your patient with severe AS a fast acting and potent antihypertensive. Could be something like IR nifedipine or a push of an IV antihypertensive agent (IV hydral I’m looking at you 🙄 🙄 🙄 🙄 🙄 🙄 )
Now, just like all of us humans, your body doesn’t LOVE change, right? It likes to keep homeostasis; it loves keeping up appearances and keeping everything stable up in there.
If you know this show, we can be friends. Also you too probably grew up without cable until you were halfway done with high school.
So you give an IV anti-hypertensive that works on vasodilating/relaxing the vessels – what factor is going to change in our BP equation?
SVR! right?
So then SVR is going to drop it like it’s hot and in order to avoid actual hypotension, what is your body going to do in response?
It’s going to have to figure out a way to increase cardiac output, right?
Now normally, the body would undergo reflex tachycardia to help compensate, get cardiac output up and preserve blood pressure.
Keep in mind that cardiac output is a measure of the amount of blood your body is getting per unit of time, aka stroke volume multiplied by heart rate.
In severe aortic stenosis, though, your aortic valve opening is literally so restricted and small, that reflex tachycardia ain’t going to increase the amount of blood leaving your heart – in other words, given the severity of the AS, your cardiac output will remain fairly fixed in the setting of a potent decrease in SVR.
What this leads to is a potentially life-threatening case of hypotension – since your body cannot compensate like it would normally do.
Because of this, we really, really, really want to avoid anything that can mess with SVR too rapidly and potently, like IV boluses of antihypertensives or fast acting oral agents like IR nifedipine.
The rule of thumb in aortic stenosis is: if we’d have to pick, we’d rather have these patients run a little high than risk dropping them too low. And that reason all boils down back to pathophysiology.
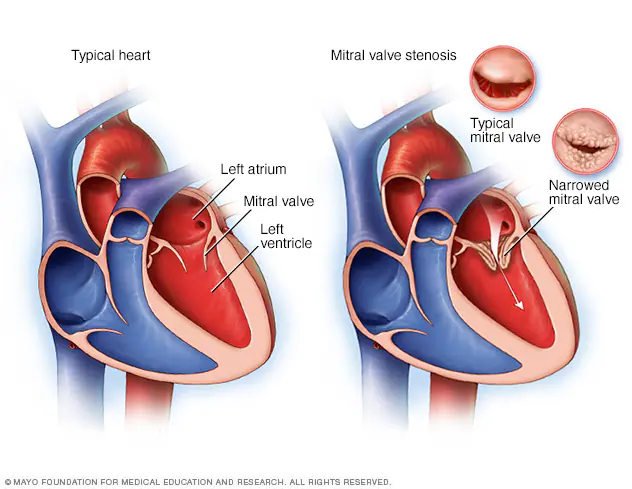
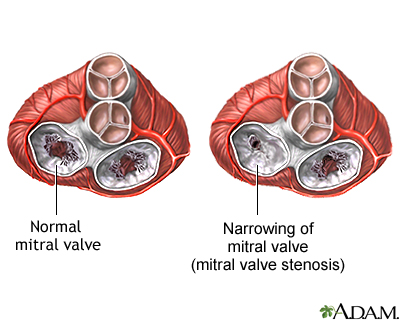
Mitral Stenosis
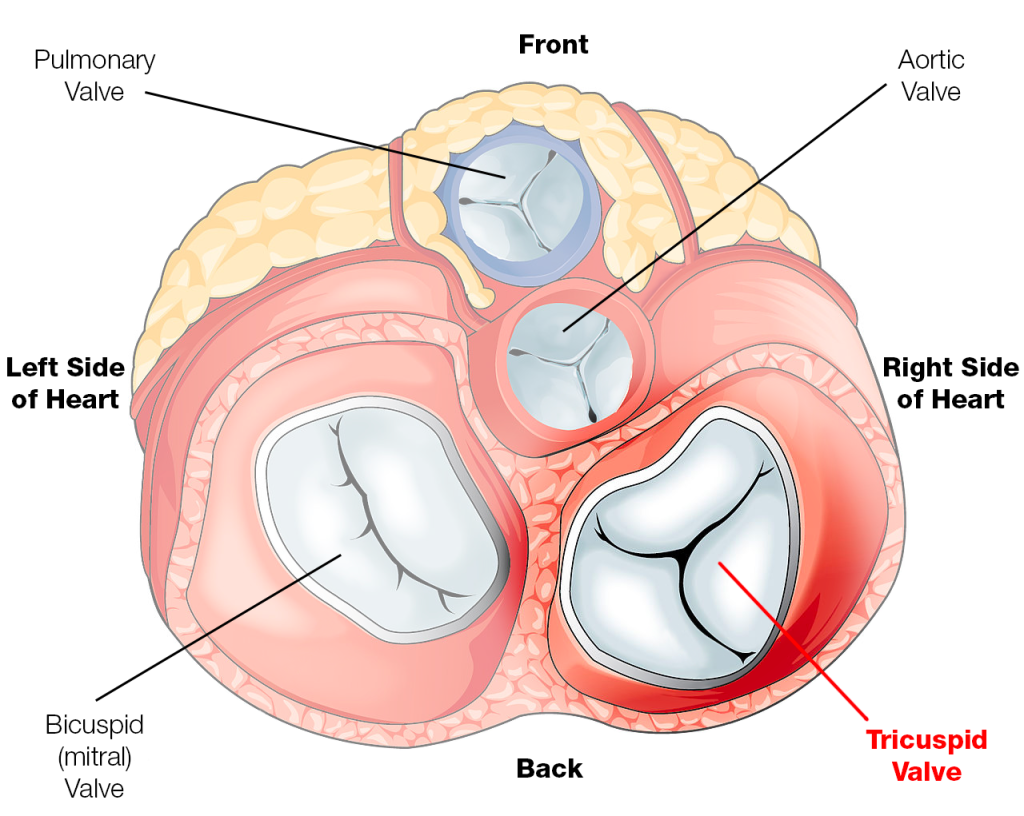
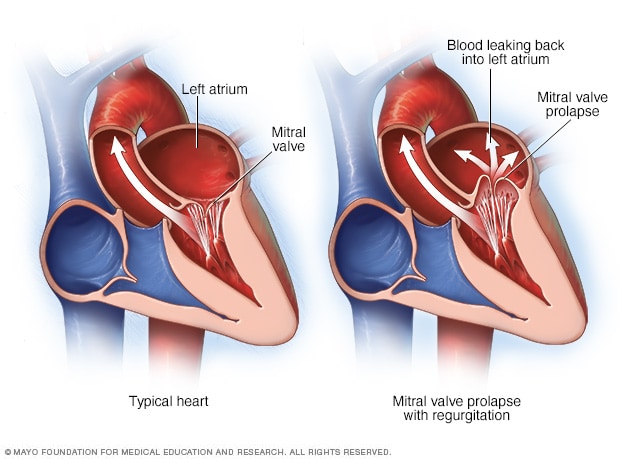
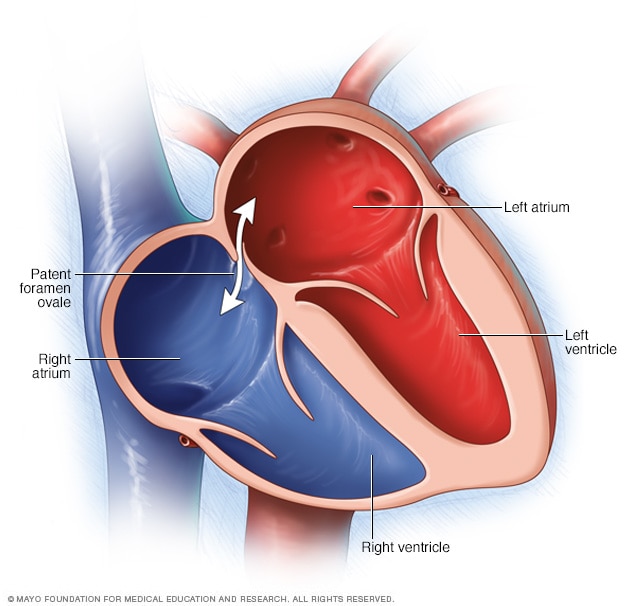
Alright next up to bat are patients with mitral stenosis, aka a really narrowed mitral valve. To reorient ourselves, the mitral valve is the valve that sits between the left atrium and the left ventricle.
Source: the Mayo Clinic
Let’s keep in mind how it feels to be the mitral valve. Very Gen Z of me I know (kidding). But seriously.
If you were standing on the mitral valve, what are you experiencing? What kind of pressures are you seeing?
‘Time to sit on the mitral valve, y’all!
If you remember from our basic hemodynamics and coronary anatomy posts, you might recall that amount of pressure the mitral valve sees is….. pretty….minimal, at least compared to the pressure that the aortic valve experiences.
Sure, there’s a lil bit of an atrial kick, but it’s minimal compared to the crazy crushing squeezing force of the LV.
The majority of blood flow movement through the atrioventricular valves (aka both the tricuspid and the bicuspid valves) is passive. What I mean by this is that the mitral valve will open – the left atrium will do a little *ehhhhh*, and then most of the blood will just flow through during that period of diastole.
DAT ATRIAL KICK DOE.
Why did we review this? It’s because the “treatment” for mitral stenosis patients draws exactly on this concept.
Again – tightened tiny narrowed mitral valve, mostly passive blood flow – what can we do to potentially increase the amount of blood that flows through the mitral valve?
Any ideas?
Two words: beta blockers.
In case you didn’t guess beta blockers – I want you to think about it – why do you think it would make sense to use beta blockers in the setting of mitral stenosis?
What do beta blockers do to our hemodynamics?
By decreasing the ability of norepinephrine and epinephrine to bind to the beta-1 receptor, we slow down heart rate.
If you slow down heart rate, you are effectively decreasing the amount of ventricular contractions per unit of time (e.g. instead of 100 beats per minute, you’re down at 60 beats per minute).
If we are decreasing the amount of time spent in systole, then we are….increasing the amount of time spent in diastole.
And by increasing the amount of time spent in diastole, or ventricular relaxation – you guessed it – we are increasing the amount of time that the blood has to passively go through that stenotic mitral valve. And thus we help increase the amount of blood that flows forward into that LV.
Aortic Regurgitation
In aortic regurgitation, the issue is that we have a leaky aortic valve and instead of getting all that blood out in forward flow, a portion of it will leak right back into the left ventricle during systole.
In order to promote forward flow, we want it to be as favorable as possible for blood to want to go into the aorta as possible, right? We want to make the forward route into the aorta enticing, make it as appealing as we can.
How can we nudge the blood to try to keep forward flow?
By decreasing the intra-aortic pressure (aka the pressure within the aorta), or afterload, we are making it as easy as possible for that blood to want to continue with forward flow.
The aorta to the LV.
And so in aortic regurg, we can opt to use vasodilator therapy to help reduce some of that hemodynamic burden in some patients, especially vasodilators that target the arteries and cause decreased afterload.
This helps by enhancing forward flow – but there’s not really good data that this actually changes outcomes.
Because of this, you only really see vasodilators recommended in severe aortic insufficiency and only long-term in patients who are poor candidates for replacement or short term to help improve the hemodynamic profile prior to replacement in those with severe LV dysfunction or with heart failure symptoms.
Mitral Regurgitation
Whenever you are thinking about adding on some meds to help out patients with mitral regurg, it’s important to first figure out what kind of mitral regurg they have.
For example – if they are mitral regurg due to a really thinned walled, structurally damaged dilated left atria, you can consider using drugs that reduce preload to help with the extent of the dilation.
If patients have both mitral regurg and classic LV dysfunction – they become candidates of GDMT for HFrEF. Unfortunately, for patients with ischemic mitral regurg, there’s not any widely accepted recs to help medically manage these patients. Like any of the other types of valvular disease, once your patient starts getting symptoms, you really should start considering replacement as a definitive treatment option.
When to consider replacement.
This is out of my wheelhouse as a PharmD (s/o to the interdisciplinary team!), but in a nutshell, there are certain things that providers want to assess before making the decision to replace a valve. We don’t want to put the patient through a ton of hassle with getting their valve removed and replaced if it’s not clinically significant. As a quick overview, there’s a few core tests that are generally used to assess these patients.
The standard diagnostic test that is generally used to evaluate these patients is the transthoracic echocardiogram (TTE).
Echos are utilized to physically see the structure and function of the heart – the chambers, the valves, the size of the aorta, etc.
Source: the POCUS ATLAS
Using fancy tools with ECHO (like Doppler ECHO), the team can determine the hemodynamics around the valve noninvasively.
Source: THE POCUS ATLAST
For stenosis, measurements like maximum velocity, mean gradient, and valve area are often taken.
For regurg, regurg orific area, volume and fraction is checked.
Depending on the severity of these measurements along with patient presentation, the decision whether or not to repair or replace will be made by the interdisciplinary team.
Definitive Treatments: Repair or Replacement!
We’ve come to the final part of our discussion on valvular disease in the heart – replacement.
For many patients, this will be their best bet at long term durable outcomes.
The landscape of valve replacement has really, really changed over the past few decades. It’s really incredible to see how far we’ve come in such a short period of time.
The History of Heart Valve Replacement
Let’s jump back into the wayback machine and head to the 1950s – really not that long ago if you think about it.
The first real kid on the block was Charles Hufnagel – a physician and a surgeon from Georgetown who is generally credited with making the first ever prosthetic heart valve.
His technique was different than what we are used to today – he created an extra valve – known as an aortic “assist” valve in the descending aorta of a patient with aortic regurgitation out of plastic. The purpose of the valve was not to replace the faulty leaky aortic valve of the patient, but rather to ensure forward flow at the point after it, preventing backflow back in the ascending aorta and back into the heart. The valve was about 1.5 inches, made of plastic, and consisted of a free moving plastic “pea” inside of a tube. That pea would be dislodged by pulsating blood with each heartbeat, closing during the period of diastole.
Dr. Hufnagel performed the first ever successful implantation of an acrylic ball valve in the descending aorta in a 30 year old female with severe aortic regurg.
The OG Hufnagel valve. Source: Wikipedia
Placement of the Hufnagel aortic assist valve (note it’s in the descending aorta, somewhat far from the diseased aortic valve).
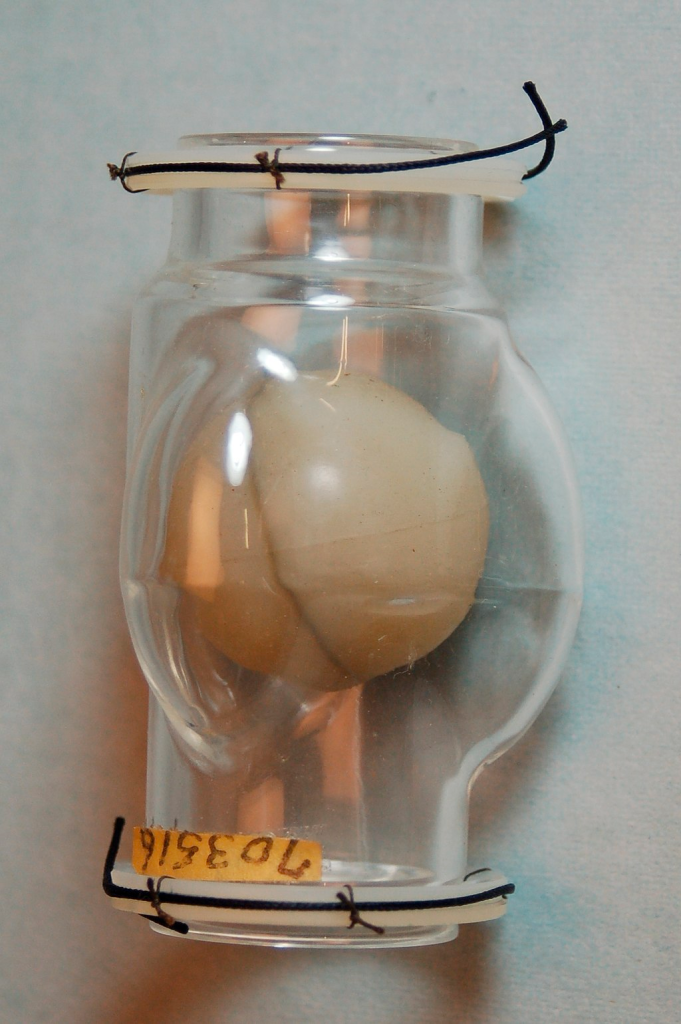
The next big pioneers included Dwight Harden, in 1960s, who invented and implanted a new type of design – known as the ball and cage heart valves (known as the Harken-Soroff valve), along with another type of ball and cage valve created by Dr.s Starr and Edwards – aptly known as the Starr-Edwards Valve.
Believe it or not, the design for these valves came from the idea of old bottle stoppers. These valves were put into the more standard position we are familiar with these days – aka in the annulus of the valve itself.
The first ever successful mitral valve replacement was performed by Starr and Edwards and their original manuscript can easily be accessed online for free.
The Starr Edwards Ball and Cage Valve. Source: Cambridge University Press
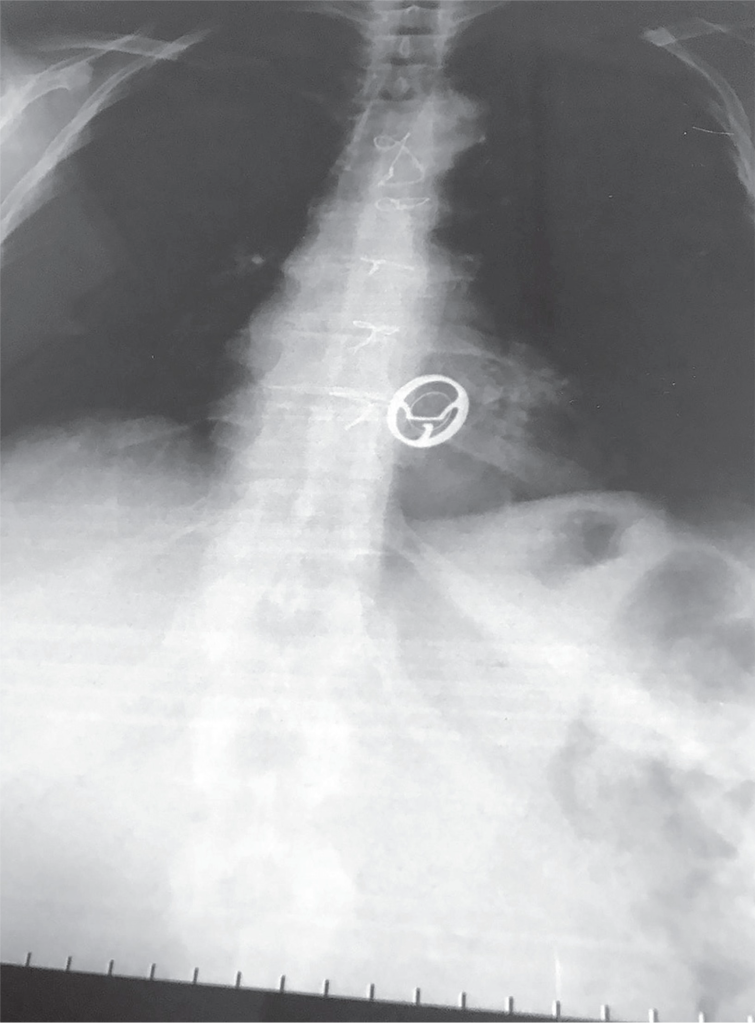
Check out that big boy! Another thing to note is the sternal wires – any patient that has had open heart surgery will end up with sternal wires that can be seen on Xray for life. Source: reddit.
Source: NJEM Group, Youtube.com
Another interesting piece of history to note is Dr. Harden – the surgeon above – started his career in the 40s by figuring out a way to treat mitral stenosis by quite LITERALLY cutting a small hole in the heart, blindly going in, and sticking his finger into the heart and literally opening up the crusty heart valve with his finger. They called this technique at the time “closed heart surgery”. Unsurprisingly, the majority of patients died in the beginning but as they practiced, the mortality rate decreased over time.
My point is – even just a few decades ago – in the lifetime of many people still living today – we were quite literally poking our fingers into hearts and wiggling our fingers around to treat patients. We have come such a long way, but it’s important to really appreciate and respect the journey that we’ve made in such a relatively short period of time.
These early ways were far from perfect – and it became clear that there was a need for surgeons to actually gain access to the inside of the heart and work from within – but they quickly ran into a problem.
If they kept circulation running, your patient would bleed to death if you tried to open up their hearts – but if you stopped circulation temporarily, you only bought yourself about 4 minutes to work before the patient started undergoing brain damage. IDK about you, but I can barely make a cup of coffee in that amount of time, let alone start and finish heart surgery.
It wasn’t until 1953 when the first heart-lung machine was introduced – by bypassing the blood from going into the heart and lungs and artificially oxygenating the blood, this made the idea of open heart surgery a reality for the first time in history. The first ever surgery was to repair an ASD (atrial septal defect) in an 18 year patient who lived over 30 years afterwards.
Before we continue on to talk about the evolution of these early valves – let’s talk about the implications that having these valves placed might cause.
If you think about it,
The ideal heart valve would be durable, physiologic, recognized as the body’s own, and have a very sleek and favorable hemodynamic profile that would mimic our natural valves.
Obviously the ball and caged valves…….are far from this. Like seriously – anything BUT sleek.
What do you think a consequence of having this foreign object valve placed into your heart?
Besides common things like bleeding during the operation or the risk of infection that comes with any large procedure, one of the biggest issues we face with artificial valves is thrombosis.
If you need a refresher on thrombosis and the clotting cascade, check out that post under archives. When an existing valve is replaced, the patient’s coagulation system will be activated on both sides – both the intrinsic and extrinsic clotting cascade.
The damage and irritation to the tissue will active the extrinsic clotting cascade (aka tissue factor will be released and the process will start up leading to fibrin formation) – and the presence of this new foreign object (the valve itself) – will activate the intrinsic clotting cascade.
Source: Teachmephysics.com
Thrombosis is therefore a big complication of getting a heart valve. Keep this in mind going forward.
Another interesting nuance about the ball and cage valves is noise – these bad boys were pretty loud as they moved back and forth.
If you are lucky enough to meet a patient that has one of these old generation valves (and yes, they are still around), you should be able to hear the ticking if you are silent next to them.
I had a patient with a Starr-Edwards Ball and Cage valve once that would joke with me that their least favorite part of the valve was that it messed up their poker game, since their heart rate would change when they got a really, really good hand. Talk about giving away your hand.
It eventually became obvious that these patients needed something to prevent thrombosis of their valves and warfarin became the standard of care. Why warfarin?
Well, warfarin was pretty much our only oral anticoagulant at that time.
With the large surface area and turbulent flows associated with the ball and cage valves, the hunt for a more streamlined, more physiologic valve was on.
Before you knew it, a new generation of valve was developed, one with a leaflet that would rotate open and close with each beat – also known as a “tilting disc” valve.
A team consisting of both an engineer and a heart surgeon (Donald Shiley and Viking Björk, respectively) came together to create the first successful-tilting disc valve – known as the Björk-Shiley valve. The valve got its feet off the ground in 1971 and was used to replace both aortic and mitral valves.
These valves made of a mixture of metals and carbon were very popular and widely used in the 1970s – however, in a few years, it became apparent that these valves had some durability issues in the long term, and could shed microscopic metal fragments. Woof.
Starting in 1979, the design was changed to help speed manufacturing and to make flow more physiologic – however, as a result, a weaker structure with more issues arose. These convexo-concave valves could fracture and cause sudden cardiac death.
Because of this, the FDA withdrew approval of the valve in 1986, and a multi-million dollar lawsuit was settled. Some patients still have this valve implanted – the decision and benefit of replacing the valve does not always exceed the risks of another open heart surgery.
Source: AHAThe shearing of the struts. Source: NJEM
The search to improve hemodynamics continued over the next few decades – landmark valves included the St. Jude Medical (SJM) bileaflet mechanical valve in the 1970s. Bileaflet valves allowed for three flow areas through the valve with a more uniform physiologic flow.
The more hemodynamically streamlined, the less turbulent, and therefore the lower the risk of stagnation and therefore thrombosis. Bileaflet valves are still used today.
St. Jude Medical Bileaflet Valve. Source: ResearchGate
Bioprosthetic Valves
But what about non-mechanical valves? There is a whole other category of heart valves known as bioprosthetic, or tissue, valves. The history of tissue valves started back in 1962, when Donald Ross performed and created the Ross Procedure, which was used for patients in need of an aortic valve replacement.
The procedure was pretty badass. The Ross procedure involved cutting out a patient’s aortic valve, and replacing it with the patient’s own healthy pulmonic valve. The empty pulmonary valve spot would then be filled by a pulmonic valve from a cadaver.
The Ross Procedure. Source: ResearchGate
Why use a patient’s own native pulmonary valve just to replace the old pulmonary valve position with a cadaver valve? Why not just replace the aortic valve with the cadaver valve? Why have the patients go through more cuts and why not just leave the pulmonary valve alone?
Keep in mind that the aortic valve has to be the toughest valve in our heart – it sits right next to the left ventricle and therefore has to tolerate the largest, toughest pressures in the body.
The idea was that a cadaver valve will be flimsy at best to start with, and would likely not be able to tolerate these pressures long term. Therefore, it was thought to use to “next best thing” – the patient’s own native valve that has to tolerate the somewhat high pressures of the right ventricle – aka the pulmonary valve. It’s not perfect, but it’s better than a dead person’s valve I guess.
However, when Ross started out trying to fix aortic valves, the cadaver valves he tried to put in……disintegrated.
In 1962, the first valve replacement from a human cadaver was done by Alfred Gunning with a cadaver valve that was previously freeze-dried. With this technique, Gunning gave some of these freeze-dried valves to Ross, who was then able to replace a valve with the patient recovering well afterwards. Fantastic!
The idea of using bioprosthetic valves – which made sense – was that “our entire physical makeup and body structures represent the end result of millions of years of evolutionary development” and that we would be unable to exactly replicate this through a (wo)man-made mechanical valve.
Because cadavers were difficult to obtain and likely costly, the search also turned to other animals, like pigs or cows. But biologic valves from other sources came with their own slew of issues – the most obvious one being tissue breakdown. Since we’re talking about actual tissue, they had to figure out a way to both sterilize and preserve tissue so it didn’t cause infection or broke down the second you put it in.
They discovered a method of preservation that helps to preserve the valve, prevent rejection, and keep calcification at bay. With these techniques, it was found that the cow (bovine) valve lasted about twice as long as the pig (porcine) valve, making the cow valve the tissue valve of choice.
These tissue valves are generally positioned on a plastic or metal thing stent covered with fabric, or can be stentless and come with a portion of the aortic root really reinforced. See some examples below:
Source: Valve-in-Valve International Data (VIVID)
Bioprosthetic versus Mechanical Valves: Who gets what and why?
Once bioprosthetic valves were introduced, there now became an option for patients – prior to their introduction, the only thing that was really available were mechanical valves.
With different choices, came measuring and weighing out pros versus cons.
Thrombosis | Need for Oral Anticoagulation
A common complication of valves in general was the risk of thrombosis. When thinking about tissue valves versus mechanical valves – which do you think would carry a higher risk of thrombosis over time and why?
Think back to the triggers of our coag cascade.
Implanting a new valve, no matter what it’s made of, will initially cause some tissue injury and endothelial damage at that site, triggering the extrinsic coag cascade. However:
Mechanical valves are foreign and made of metals, and so with them comes a big risk of thrombosis. Additionally, the body never will fully accept and endothelialize that valve, and so a portion of it will always remain available to the bloodstream and be a risk factor for thrombosis.
Meanwhile, tissue valves still carry a risk of thrombosis but it is much, much lower. Over the span of a few months, your body will start to endothelialize over that valve and incorporate it into the wall of the heart (in a process very similar to coronary artery stenting – check out the ACS posts if you are confused).
Because of this, patients who receive a mechanical valve immediately buy themselves lifelong anticoagulation. In contrast, patients who receive bioprosthetic valves either do not need OAC at all or may just do a short term course, depending on what valve is replaced (we’ll get to this later).
Because of this, in patients who have high bleeding risk factors, a tissue valve may be better for them.
No matter what type of valve your patient gets – whether bioprosthetic or mechanical – whether in the aortic or mitral position, some antithrombotic therapy will be needed – but lifelong OAC is really reserved especially for those with mechanical valves.
Durability
Bioprosthetic valves versus mechanical valves also have very different “life spans”. Mechanical valves are ….. mechanical!, therefore once you get one, it should really last lifelong (unless you encounter other complications).
However, once a tissue valve is put in, you really only get a good 15-20 years out of that valve if you are lucky, and may be even less than that.
Who gets what:
This is a generalizability and not true for all patients, but usually the really old patients or really young patients are a little bit more “clear cut”.
In our very old patients, we will likely opt to do a tissue valve. This way, they won’t need to be put on long term OAC (and keep in mind the elderly tend to have increased risks of bleeding as well as well as falls) and chances are, that tissue valve will last them the remainder of their lifespan.
In our very young patients, we often will STILL opt to do a tissue valve. Why? Again, a generalizability, but often younger patients tend to be more active, involved in more “dangerous” activities (like climbing up ladders or playing football).
Because of this, we wouldn’t necessarily love to commit them to LIFELONG oral anticoagulation from the start. By implanting a tissue valve, we give them another 15ish years without committing them to anticoagulation and then the idea is by the time that valve is spent, they will still be well and young and healthy enough to get another sternotomy (if need be).
The middle aged patients may often be the hardest to decide on. Other factors to consider in these selections are patient occupation (e.g. sits at a desk all day versus…..a lumberjack), compliance (because if they don’t want to take OAC, that valve has a high risk of clotting up), etc.
The Operation Itself
Not a lot to say on this (clearly not in my wheelhouse as a clinical PharmD), but hopefully it makes sense that if a surgeon is replacing a valve, your patient 110% has to be put on cardiopulmonary bypass. This should make sense, since the surgeon literally has to cut directly into the heart to access the valve. If blood was still flowing through the heart – well, your patient would die on the table and bleed out pretty quick. And so they bypass the heart and the lungs, and stop the heart.
The surgery is also super interesting – if you ever have a chance to observe one, I highly highly recommend it. I have a ton of respect for CTS surgeons in general and especially considering the amount of dexterity they need to sew these valves in.
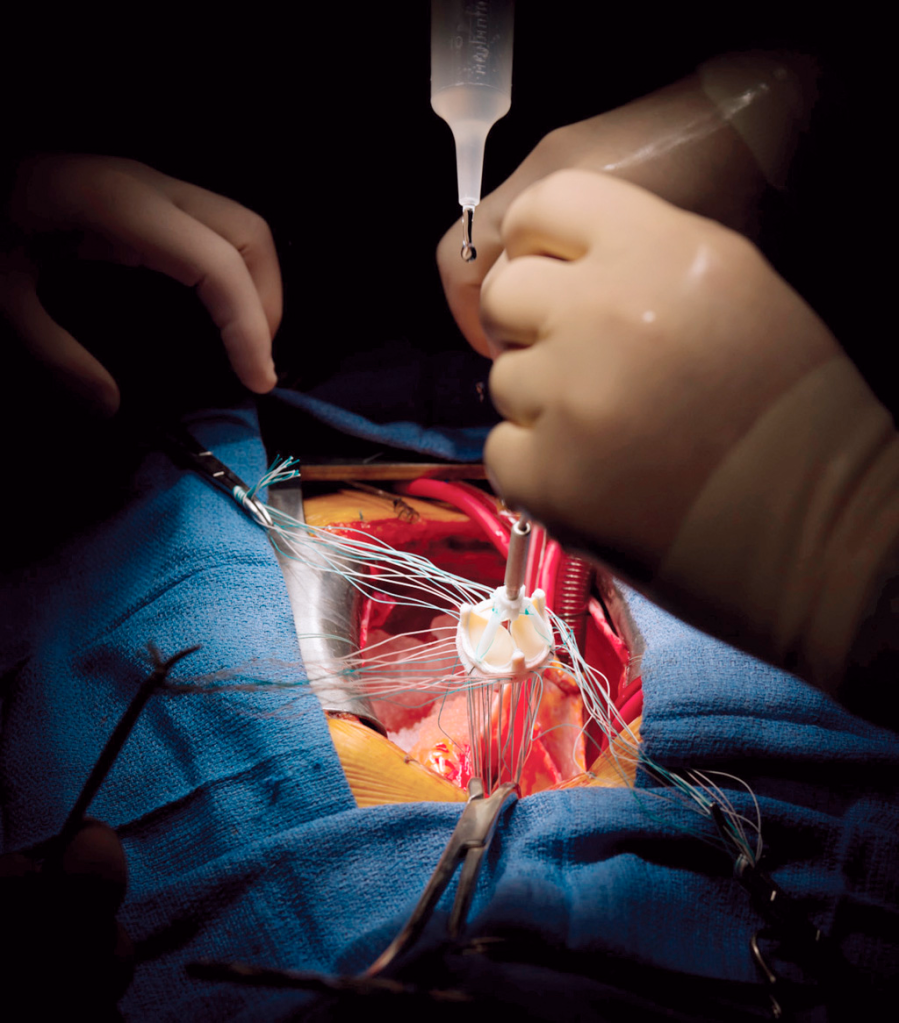
CTS surgeons will basically take out the existing valve, start suturing up the new replacement valve outside of the chest cavity before slowly sliding it into place and finishing up the sutures. Like can we appreciate the amount of stitches and handiwork these people have?! They must be really good at stitchwork/embroidery too if they put their minds to it.
Like do you SEE the amount of stitches?! Source: Modernhealthcare
Pharmacotherapy After Surgical Valve Replacement
Alright my friends. Next up we have to talk antithrombotic regimens. We already know that mechanical valves have a higher risk of thrombosis with them, and with that – a lifelong ticket to oral anticoagulation. But does the degree of anticoagulation differ based on which valve we’re replacing?
And what about bioprosthetic valves? You’re still cutting into the valve area and leaving in a semi-foreign object (afterall, it’s usually made from a cow) – these should theoretically activate both the intrinsic and extrinsic coag cascade.
Let’s talk through the two most common valve replacement positions: the aortic valve and the mitral (bicuspid) valve.
Try to think your way through this: which valve position do you think has a higher risk of thrombosis?
Need a hint? First think about the factors that influence thrombosis and clot formation in general.
The big three that we usually think about are: stasis, hypercoagulability, and injury.
In theory, both positions – whether the mitral valve or aortic valve – should undergo a similar degree of tissue injury during the procedure. No matter what the position, the surgeon still needs to cut out your defective old valve and suture in a new valve.
Now what about the amount of stasis these valves go through?
We’re going to Magic School Bus Miss Frizzle this.
Once again – imagine yourself hanging onto that mitral valve in the left atrium. The mitral valve sits between the left atrium and the left ventricle.
Source: Mayo Clinic
What kind of pressures and blood flow are you experiencing? In order to think about this, keep in mind what normal heart function looks like. If you remember from our core talks, you’ll remember that – sure there’s a lil bit of an atrial kick as the atria depolarize, but the majority of blood flow from the atria to the ventricles is passive – in other words, the blood moves on its own simply due to the AV valves being open.
Honestly, thank god this is the case because if we really relied on atrial contraction for perfusion, patients in AF would be in a lot of trouble.
Anyway, on that mitral valve – you’ll likely not experience super high, fast pressures and blood flow movement. At least relatively speaking.
Now let’s Miss Frizzle the aortic valve up in here. Imagine you are sitting on the aortic valve.
Source: Mayo Clinic
Keep in mind the aortic valve is aptly named since it sits between the LV and the aorta. What kind of pressures is the aortic valve experiencing compared to the mitral valve? High? Low? The same?
Waaaaaaaaay higher. The LV is the workhorse of the heart – the Dwayne the Rock Johnson of those chambers. It is meant to generate high contraction and high pressures.
Because of this, valves in the aortic position are less likely to form clots compared to those in the mitral position. Afterall, the aortic valve is seeing higher pressure/flows and therefore the blood there experiences less stasis. Less stasis = less thrombotic risk.
And so – keep this in mind when we discuss antithrombotic agents post surgical valve replacement.
Let’s start with mechanical valves. As we talked about above, these patients need oral anticoagulation lifelong because that valve never completely endothelializes and becomes accepted as our own.
We know the only main oral anticoagulant we had was warfarin. And for years we have nothing else we could give orally. Untilllllll…..
In the 2010s, we finally had the introduction of the direct oral anticoagulants – the DOACs.
The DOACs were a very exciting time for cardiology history – after all, for the first time we had medications that had lower risk of intracranial hemorrhage, are taken orally, and didn’t need frequent INR monitoring.
But in order to really see if they are efficacious in this patients population – we have to study them.
Cue the REALIGN trial.
The REALIGN trial was conducted in 2013 and sought to answer the question – can we use DOACs instead of warfarin in patients with mechanical valves?
And so this 2013 trial looked at dabigatran versus warfarin in patients with mechanical heart valves.
Aaaaaaaaaaaaaaaaaannnnnnnnnnnnnnndddddd….
The trial had to be stopped early due to an excess of both thromboembolic AND bleeding events in patients in the dabigatran arm. 😭😭😭😭😭😭😭😭😭😭
A sad day for medicine.
Because of this, if you check out any valvular disease guideline, you’ll see that there is a class III (harm) recommendation that you cannot and should not use dabigatran in patients with heart valves.
What about the other DOACs you might ask? Well, for one- I’m not sure I would be the one brave enough to retrial this with another DOAC in this same patient population.
In a few minutes, we’ll get to a more recent trial that studied another DOAC in patients with a very specific types of heart valveand whether the decision to use DOACs in patients with mechanical heart valves has changed.
But for now – for the most part – warfarin it is. She ain’t going anywhere anytime soon.
However, the INR goal is going to depend on where the valve location is. Since the mitral valve is more thrombotic of a position than the aortic valve for reasons listed above, theI INR goal is higher in mitral mechanical valves (in other words, we thin out these patients’ blood MORE).
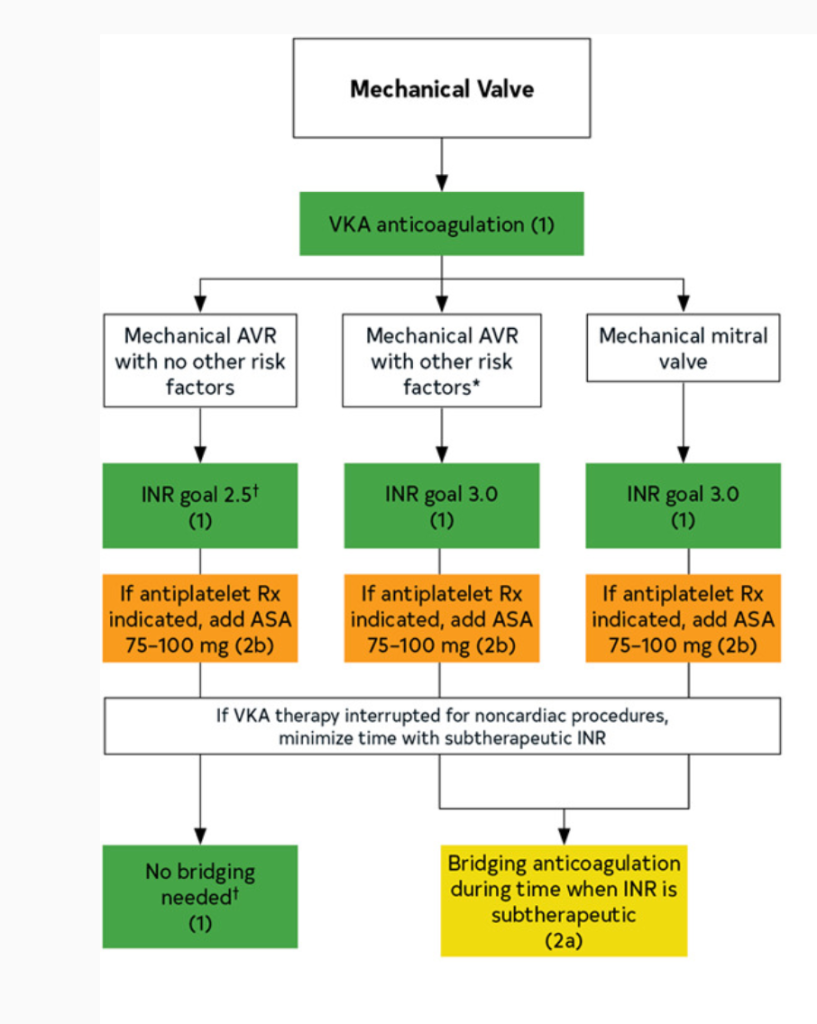
In patients with mechanical heart valves, all need lifelong warfarin. However:
Mitral mechanical valve: warfarin with INR goal 2.5-3.5 indefinitely
This is the “standard” treatment for most patients.
Special Populations:
If you look at the 2020 American disease guidelines, you will notice that a higher INR goal can be considered if a patient has both a mechanical heart valve and other risk factors for thrombosis.
These all include patients who are more likely to form clots at baseline, such as patients that also have atrial fibrillation, other hypercoagulable states, really bad systolic heart failure (remember – low squeeze means higher risk of clot!), or in patients that have older valves (like that ol’ hunk ball and cage ones – since those are old and have such a high surface area, we usually will do 2.5-3.5 for these patients.
Lastly, in select patients, you may opt to add on a baby aspirin in addition to the warfarin therapy above – however, this is really for patients that have another indication for baby aspirin (e.g. hx of ACS, PCI, etc). Since they are already being fully anticoagulated, the decision should be made with care based on your individual patient.
Straight from the 2020 ACC/AHA Valvular Disease Guidelines
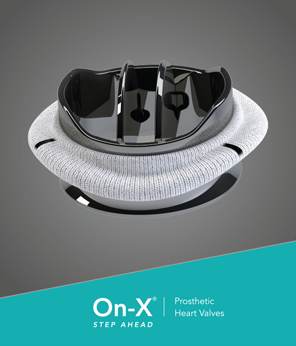
Before we move on to bioprosthetic valve care, there’s one special type of mechanical valve we need to talk about first. It’s known as the “On-X” valve.
Keep in mind the big “con” that comes with mechanical heart valves is the need for full-intensity anticoagulation with warfarin.
So it would be in a company’s best interest to figure out a design of a valve that decreases the rate of thromboembolism and either eliminate the need for OAC (unlikely) or at least lower the “intensity” of warfarin therapy needed.
Cue the On-X valve. (i’m not sponsored i swear (but if anyone wants to pay me hit me up, I’m good 4 it)).
The ON-X valve. Source: Cryolife
The makers of the On-X valve believed that their special valve had a lower risk of thrombosis when compared to the other available types of mechanical heart valves.
And so they put their money where their mouth was and did a trial to see if patients with this special valve would be able to get away with lower intensity of warfarin anticoagulation.
This was studied in the 2014 PROACT Trial.
And – they found that lower intensity warfarin did not carry a higher risk of thromboembolism, and also had a significantly lower risk of bleeding. WAHOOOOOOOOOOOOO! But wait:
A few key things to note about this trial:
They only studied patients who received the On-X in the aortic valve position
All patients were required to be on standard intensity warfarin therapy (e.g. INR 2-3) for the first 3 months after implantation; afterwards, patients were randomized to either standard intensity therapy (keep INR 2-3) or lower intensity warfarin (defined as INR goal of 1.5-2).
All patients were required to be on baby aspirin (81 mg/day)
Why are these things pertinent?
The first point – that only AVRs were included – makes sense, especially from a harm standpoint. We know AVRs have a lower thrombotic risk than MVRs and so it would make sense the first step to “get your feet wet” to see if lower intensity would be ok would be to study it in the lower thrombotic risk group.
With that being said, in my opinion these results would not be translatable into valves located in the much more thrombotic mitral valve position.
It’s interesting to note that they didn’t lower the intensity of anticoagulation until 3 months in. Any guesses as to why?
It’s likely because the immediate post-op period comes with the highest risk of thrombosis – over those first 3 months, you are letting the sutures heal and allowing that heart to settle. Once this period passes, your risk of thrombosis is lower. It makes sense that the company funding this trial might want to “cover” patients during this acute period with normal intensity so that they didn’t see a large uptick of thromboembolic events in these patients.
Because of this, in practice, we follow what was done with the trial – and drop the intensity on anticoagulation once you are 3 months post procedure.
And lastly – all patients were on baby aspirin in addition to their aspirin – which is not typically done for your standard patient without any other indication for aspirin. Any ideas why they did this? They probably were worried about extra thrombosis in the lower intensity experimental group so by adding aspirin to ALL patients, they could cover some of this risk while not making the experimental group have a higher risk of bleeding (since even the standard intensity warfarin group had baby aspirin on board).
Long story short – in patients that have mechanical On-X AVRs, we follow this trial and do 3 months of standard warfarin therapy plus aspirin followed by lowering the intensity of warfarin 3 months in to 1.5-2 and keep that baby aspirin on board.
What about the mitral position?
We know that the mitral valve position is more thrombotic, so if the AVR On-X fared well, I think a reasonable question is what about the MVR On-X?
They redid this trial in the MVR position (the PROACT Mitral Trial)- and, initial data was promising. However, the paper was retracted due to issues with stats and when it was reprinted, the lower intensity warfarin did not achieve noninferiority versus standard dose warfarin. Bummer. Too good to be true.
But…..the question of DOACs arises in mechanical valves….again…..
Alright so we’re out of luck for the mitral On-X, but we know that patients with the aortic mechanical on-x valve can be safely managed on a lower intensity of anticoagulation with warfarin.
Knowing that these specific type of mechanical aortic valves are less thrombotic than your standard valve…..it makes sense that the idea of DOACS might want to be rechallenged. After all, the 2013 RE-ALIGN trial that made dabigatran contraindicated in mechanical heart valves looked at more thrombogenic valvesand included both mitral and aortic positions.
And so they tested apixaban in these special On-X valves in the aortic position.
Cue the PROACT Xa trial.
They controlled for as many thrombogenic factors as they could – they made sure all patients had an On-X valve and only in the aortic position; they made sure patients were not switched to a DOAC until at least 3 months post implantation. They had a primary efficacy endpoint of valve thrombosis or valve related thromboembolism.
And.
The.
Trial.
Had.
To.
Be.
Stopped.
Early.
😭😭😭😭😭😭😭😭😭😭😭😭😭😭😭😭😭😭😭😭
After 863 patients were enrolled, they had to stop the trial early due to an excess risk of thromboembolism with apixaban, and this is even with 94% of patients also taking aspirin.
In summary, it sounds like DOACs are not going to be an option any time soon for the thrombosis prophylaxis for mechanical heart valves. The PROACT-Xa trial really further cemented this idea.
Alright! We finished up with the mechanical valves, now let’s talk about what happens to patients after they get either a mitral or aortic bioprosthetic valve placed surgically.
We already discussed how bioprosthetic valves are a lot less thrombogenic. This is because they are more similar to our native tissue and within the first 3 months after implantation, most of that valve gets endothelialized over and accepted as our own.
Bioprosthetic Aortic Valve Replacements
In the aortic valve position – with high flow and high pressures – your risk of thrombosis is fairly low. Because of this, patients who get a bioprosthetic aortic valve only need to be managed with baby aspirin lifelong. That’s enough to cover them from clotting off on this new tissue valve.
The mitral position is a little more hairy – after all it is seeing lower pressures, slower flow. Because of this, some extra coverage is needed during those first 3 months while the bioprosthetic valve settles into its new home in the mitral valve position.
In general, for patients who end up getting a surgically-implanted bioprosthetic (tissue) mitral valve, because of the higher risk of thrombosis, warfarin is given but only for the first three months. This should make sense – we’re going to help support that valve as it goes through the process of endothelialization – after that, the risk of thrombosis is greatly reduced. After that 3 month mark, we will generally drop the warfarin and transition to just a lifelong baby aspirin 81 mg.
ESC 2021 Valvular Dx Guidelines
Alright. That was a lot today. Phew. Thanks for hanging in.
Next post will focus all about a newish spiffy technique known as TAVR. It involves valve replacement without your typical cardiothoracic surgery techniques (all done via catheter).
Welcome back, guys! Today we are going to start our journey into ✨valvular heart disease✨. This is a very, very pathophys heavy topic, and if you follow along, hopefully you won’t have to memorize anything because the pathophys will make sense. Because this is so pathophys heavy, we actually won’t even be talking about treatments until next time.
I think the biggest thing to focus on when we discuss pathophys is just the ability to slowly follow along and be able to understand each step that happens. You might not be able to recite the pathophys off the top of your head anytime soon, but hopefully you will have an appreciation for the effects of valvular heart disease and also what is actually happening in that heart.
My goals for you are to understand what these valves look like when we say the words “stenosis” or “insufficiency” or “regurgitation” and realize why the heck these valve issues can become so important that we actually perform open-heart surgeries in these patients on bypass.
This is definitely one of our more dense discussions, so if you’re too tired to hang right now, I recommend coming back when you are feeling a bit more refreshed (think of this post as watching “The Last of Us” instead of just casually half-watching the episode of Seinfeld you’ve seen 10,000 time in the background).
sorry couldn’t help myself
Without further ado – as always, we’re going to start with the basics.
What valves do we have in the heart? (the main 4)
Let’s get you oriented again. If you need a better refresher on anatomy, check out the “coronary anatomy overview post.
We got ✨4✨ main valves in our heart.
If we follow our typical blood flow route, our deoxygenated blood enters the right side of the heart, from the vena cava into the rightatrium.
From the right atrium, blood moves through the tricuspid valve into the right ventricle.
The right ventricle squeeeeeeezes that blood through the pulmonary valvewhere blood then enters pulmonary circulation.
Once oxygenated, this blood flows into the right atrium, through the mitral valve to the left ventricle and finally out the aortic valve on its way to provide your body with nice oxygenated blood.
Check out the diagram below to follow along.
Source: Wikipedia
Luckily for us, I’d argue that two of these valves have really easy to remember names (we love that for them):
The pulmonary valve is the one that is our gateway to the pulmonary circulation, while the aortic valveserves as the gateway to the aorta and out to the rest of the body.
That leaves us with the tricuspid and mitral (aka bicuspid) valves. These can be grouped together as our AV valves – aka our atrioventricular valves, aptly named because of their place in the heart (again, we love when names make sense).
Source: DifferenceBetween.com
The mitral valve is also known as the bicuspid valve.
The AV valves in action! Source: Kietil Lenes
The bicuspid and tricuspid valve are aptly named because of how many leaflets they are supposed to have – with tricuspid having 3 and bicuspid have 2. Check out that figure above to visually see what I mean, and that gif to see them in ✨action✨.
Fun fact: Do you know why we call the bicuspid valve the “mitral valve”?It all goes back to its apparent resemblance to the mitrehat that bishops wear. (I guess I can kindaaa? see it)
source: liturgical vestments
You can remember this however you want to. This may not help ANYONE so feel free to disregard: I personally am not the most religious person, but when I was trying to memorize the names of the valves and their respective sides, it helped me to mentally associate this idea of the mitral valve being associated with something religious. Bishops are often seen as important within their religious congregations, and so the mitral valve must be on the tougher, stronger, “more-important” side of heart – the left side.
As you may remember from our core discussions that the left side of the heart – specifically the LV is generally regarded as the more powerful/stronger side (cue flashbacks of Dwayne the Rock Johnson). This is how I remember that the mitral valve is on the left side of the heart and the tricuspid on the right.
Our aortic and pulmonary valves are known as our 🌙semilunar🌙 valves🌙. Both of these have three leaflets, are are named semilunar due to the resemblance of each leaflet to a half moon🌙🌙🌙🌙🌙.
Low key always thought about what would happen if these valves just look like something different. Like idk, a pickle. Would the names reflect that? The pickled valves? Idk. Unclear.
(For the record, we also have other valves in our heart – like the coronary sinus valve or IVC valve – but these aren’t really often discussed/applicable clinically)
Ok, now we got the names and locations down. But why do we even have valves? How do they work?
It’s a good question. The whole reason we have heart valves is to prevent backflow of blood and to ensure forward flow. In other words – we want the blood to go forward, and to make it all go blood to flow in one direction.
Trying to relate to the Gen Zs here. Bear with me. (anyone get it?) halp.
Knowing this, the AV valves (aka the mitral and tricuspid valves) prevent the backflow of blood from the ventricles into the atria, and the semilunar valves (aka the pulmonary and aortic valves)prevent backflow of blood from either the pulmonary artery or the aorta into the right or left ventricle, respectively.
Check out those bad bois go! Ey ey eyyyyyyyy! Source: Wikipedia
I feel like there is a common misconception that your valves themselves do the work of the opening and closing of them. That’s actually not the case.
The opening and closing of the valves are completely caused by the change in pressures during systole vs diastole.
What causes this? Why does this happen?
It might sound obvious, but whenever the pressure behind a valve is greater than the pressure in front of the valve, the valve will be blown open.
However, when the pressure in frontof the valve is greater than the pressure behind the valve, that valve will be pushed closed and blood flow between chambers stop.
The ventricles to the atria as they start contracting: BOI BYEEEEEEEEE
So the pressure itself takes care of the opening and closing themselves – but what’s to prevent those valves from protruding/ballooning backwards (aka prolapsing)? Afterall, these valves are just made up of flexible-ish tissue.
When it comes to your AV valves, these mitral/tricuspid valves are connected by these “chords” or strings called the chordae tendineae – aka…your literal “heart strings” (if only all these country singers knew they were talking about good ol’ chordae tendineae in their songs).
The chordae tendineae are these inelastic strings/cords of fibrous tissue that grow out of each ventricle and attach and anchor the valves into place.
These chords help keep the flaps of the valves from prolapsing when systole happens. I kind of think of them like literally strings anchoring the valves and giving them more tension as they close and open.
IDK why, but something about the chordae tendineae always gave me the heebie jeebies. Source: Wikipedia
ALLLLL the structures!!! Source: Wikipedia
Attached to every chordae tendineae are papillary muscles. Their job is just to create even more tension to help the chords do their job. The chordae tendineae + the papillary muscles together are what we call the “subvalvular apparatus”.
Now you guys know I’m a very visual learner, so just in case you needed a visual about what I mean about “valve prolapse” – here it is.
Source: MayoClinic
This can also be seen IRL in this ECHO example as well:
Source: MyHeart
Heart Valves and their Sounds🎵🎵🎵🎵
I feel like a lot of us might be familiar with the stereotypical “lub”and“dub” heart sounds, but have you ever thought about what is actually producing these sounds?
Well, spoiler alert – it’s the opening and closing of the heart valves that makes these sounds.
The closure of the AV valves produces the “lub” sound. This is also known as the first heart sound and also as the S1 sound.
The closure of the semilunar valvesproduces the “dub” sound. This is known as the second heart sound and also the S2 sound.
This is why things like heart murmurs (aka extra whooshing/swishing sounds that can be heard via stethoscope) can indicate abnormal blood flow over a valve, and prompt more investigation like an ECHO to see if there are any issues with those valves. Very often these murmurs are the first sign that physicians might notice that may indicate you may have valve issues. This is part of the reason why all doctors always listen to your heart sounds during your yearly physical.
Lub Dub, Lub, Dub. Source: QUIZIZZ.com
I think in scenarios like this, it is even better to hear and see an actual video illustrating what I mean. If you’re interested, the below is awesome:
Alila Medical Media
Stenosis, Regurg, Insufficiency, Oh My!
Just like anything else in the world, your valves can also have issues with them. Heck, you can even be born with issues with them.
The main issues we will be focusing on today are called valvular stenosis and regurgitation (also known as “insufficiency”).
Let’s first define what these words even mean.
Whenever you hear the word “stenosis”, I want you to think of a narrowing.
I used to think/associate “stenosis” with the idea of being calcified and crusty (like my 8 year old dog Luna). While stenosis can be due to or associated with calcifications, the term stenosis itself just means a general narrowing.
Luna in all her crustiness glory. My stinky girl.
When you hear the term regurgitation, think about backflowing.
Gross example – I know, I know – but another word for vomiting is regurgitation, and although gross, it’s actually pretty spot on, since your stomach contents are meant to be pushed forward into the small intestine, not backup into the esophagus and beyond. OK enough vom talk, I’m getting nauseous just thinking about it (I alway say I’m a sympathy vomiter – if someone starts even dry heaving near me I will do the same).
There are a bunch of other potpourri issues with valves that can occur and include things like endocarditis, which is a whole other thing that we won’t be getting to yet (but maybe one day).
Lastly, we also have things like congenital (aka you are born with it) valve issues that can cause problems down the line, like a patient being born with a two-leaflet aortic valve instead of the standard three. This one will be closely tied into our discussions today.
Stenosis: In General
Let’s start with stenosis. Keep in mind that stenosis means a narrowing, so in this case we are talking about a narrowing of the valve. As you guys know by now, I’m visual so let’s actually see what we’re talking about here. Let’s use this aortic valve as an example below.
Source: AHVC
A healthy aortic valve should be soft, pliable, supple (sounds like we’re describing a boob job but bare with me). When it opens, it should open fully. However, in patients that get valve stenosis, their valves become hardened, crusty, stiff. This leads to an incomplete opening of the valve, so instead of getting a huge area where your left ventricle can easily pump blood out – your poor LV has to push extra hard to generate the pressures high enough to get blood through. Check out the difference in the animation below.
Source: GFYCAT
In today’s post, we’re going to discuss both aortic valve stenosis and mitral valve stenosis.
Why do patients get valvular stenosis?
Because this is a disease that is commonly due to calcification, hopefully it makes sense that the biggest risk factor/patient population we tend to see valvular stenosis in is elderly patients. This is because it takes time for calcium deposits in the blood to slowly drop off onto the surface of that valve and get it all crusty and narrowed. Similar to a lot of patients with afib, age is a huge risk factor for the development of valve stenosis. Check out the graph below to really get a visual of what I’m saying.
Source: Edwards Lifesciences
Besides older age, other risk factors include patients with diabetes, high cholesterol levels, and hypertension among some others. Another big risk factor is being born with congenital valve defects like we discussed above. Some patients are born with valves that have the “wrong” # of leaflets (e.g. bicuspid aortic valve instead of tricuspid). Because of this structural change, we often see these calcium deposits build up in these patients at a younger age.
An example of a bicuspid aortic valve. Source: MedlinePlus Medical Encyclopedia
Ok so my patient’s valve is a little crusty – why does it matter?
As we know in medicine, sometimes there are abnormalities with things but they may not be clinically relevant – so why do we potentially subject our patients to literal open heart surgery and bypass to replace these valves? What’s the big deal?
If severe enough, valvular stenosis is unfortunately a very big deal. To illustrate why, let’s delve into specific examples – aortic valve stenosis and then mitral valve stenosis, and what can happen if untreated.
Aortic Stenosis
Pathophys
Let’s talk about aortic stenosis first. First things first, as a refresher where is the aortic valve?
The aortic valve is a three-leaflet valve located between the left ventricle and the aorta. If this info is all news to you, definitely check out the coronary anatomy overview in the foundations section.
So in this scenario, instead of having a nice pliable open aortic valve, your valve is going to be very tight and narrowed – and the amount of space the blood will pass through will be very restricted.
What effect do you think this will have on the heart? Specifically on that left ventricle?
Now, instead of having a nice wideopen valve for that LV to squeeze that blood through, imagine that LV has to squeeze all that blood out a teeny, tiny cocktail straw.
Source: Huffpost
What kind of effect is that going to have on the left ventricle?
Let’s use a real-life example. Have you ever tried to blow air out of a normal sized straw or even like a smoothie/ICEE/boba straw? It’s not too hard, and it’s pretty easy to get the air out of your mouth/cheeks and through that straw.
Well – have you ever tried to blow air through a teeny tiny cocktail straw?
Source: RegalBeagle Store
How does that feel in comparison? Is it easier? Or harder? What happens if you keep having to blow air into there for a whole minute?
Idk about you, but my cheeks start hurting when I try to blow through a cocktail straw, because it’s much much harder to get that air through.
This is because as thespacegets smaller and smaller, the pressure behind it will get higher and higher.
This is exactly the same principle that we discussed in the foundations talk on BP – the smaller the space, the higher the pressure.
If you really think about it, severe aortic stenosis is essentially the same as having a very high afterload on your LV. Except instead of hypertension being the culprit, the culprit is actually a stenotic aortic valve.
What effect is that increase in pressure going to have on that LV? In order to answer that, you have to think back to your fundamentals: are ventricles made to withstand high pressures? How do they compare to the atria?
Just like Guardians of the Galaxy Chris Pratt, your ventricles can tolerate high pressures – they were physiologically built different than those wimpy atria because they have a much tougher job to do.
But what’s going to happen over time if your LV has to handle higher-than-normal pressures? What is going to happen when it is going to consistently work harder to keep forward flow?
I’ve said it a million times, but your heart is a muscle. If I went to the gym (which I don’t) and lifted a bunch of weights and worked out my biceps – what would happen over time? My biceps would grow and I’d get jacked.
Your heart isn’t any different – in aortic stenosis, over time, that hard-working LV is going to start hypertrophying and growing and growing.
And what do you think will happen as a result if that LV continues to grow and hypertrophy? (hint hint, it has to do with the amount of space in that LV)
If you said heart failure, you’re right. Specifically HFpEF or diastolic heart failure. That LV is going to get smaller and smaller as that muscle gets bigger and bigger, until eventually your patient will start developing heart failure. And unfortunately, structural changes like that are very hard, if not impossible, to reverse.
And if that muscle continues to grow, keep in mind the amount of blood that is supplied to it by the coronary arteries are somewhat fixed. There might come a point where the muscle layer is so thick, you aren’t getting adequate blood supply to feed all that muscle. And as a result, your patient may developed combined systolic and diastolic heart failure over time. Diastolic heart failure – because that LV space is so tiny – and systolic heart failure, because some of that tissue is now dying out because it’s not getting enough blood supply. Not good.
Symptoms
Now that you know a bit about the pathophys about what’s happening in AS (aka aortic stenosis) – what symptoms do you think patients might get with it?
The thing about a lot of these valvular problems is that oftentimes patients may not have *any* symptoms until the valves get really junked up. That’s because like we said, that LV is able to compensate in the beginning.
Realistically patients with mild AS may not have any symptoms and have no idea they have any AS. This is really a disease (for most patients) that is slowly progressing over decades, as those calcium deposits get on that aortic valve. Patients only start developing symptoms once the heart’s ability to adapt is just exhausted (I kinda think about this like the myth of Sisyphus rolling that rock forever up that hill).
However, as that AS gets worse and worse, patients will start to become symptomatic. The first symptoms will usually happen only on exertion since that LV is able to compensate when the heart is chilling and not overworking – but when that heart rate picks up and more and more blood needs to be sent out to the body, that LV will struggle pushing that blood out of a literal cocktail straw. Commonly patients endorse things like chest pain (angina), syncope (fainting), shortness of breath on exertion.
So oftentimes patients will present with new complaints of shortness of breath on exertion.
Overtime, if untreated, that patient will quite literally develop heart failure and so at this point symptoms can really happen at any time, depending on the degree of structural damage. Occasionally, it will become so severe that the LV can’t handle those high pressures anymore, and you’ll start to see some enlargement/build up of pressure within the left atria.
Mitral Stenosis
OK! Now that we’ve got AS under our belt – let’s talk about mitral stenosis. And honestly, the same, core concepts apply here too. As long as you have an understanding of the valve location, and the physiological workload of a typical atria vs ventricle you can reason your way through mitral stenosis as well.
First thing’s first: where is the mitral valve?
The mitral valve is located on the left side of the heart, and sits between the left atria and the left ventricle. It sees blood from the LA, and allows that blood to flow into the LV.
Now imagine that that mitral valve is all crusty and super tight and small. The same concept here – the pressure behind that valve is going to start getting higher and higher. Where is that pressure going to build up? In what chamber of the heart? And is this chamber used to high pressures? Can this chamber tolerate high pressures?
Source: Wikipedia
Given the location of the mitral valve, if there was stenosis of that valve, we’d see a backup in pressure within that left atria. Now, if you remember from our foundations talk, the atria just aren’t really built to withstand high pressures. Afterall, their job is pretty low-key – they just have to move blood through 1 valve, and..that’s really it.
Sure there’s some contract of the atria (known as atrial kick), but it’s really minimal compared to the ventricles. In fact, most of the blood flow from the atria to the ventricles is actually passive– what this means is that the valves open, and really just the presence of the valve being open allows the blood to move on through to those ventricles.
Because the atria aren’t built to push against high pressures and compensate and get super jacked, what we see in mitral stenosis is a ballooning of that pliable left atria as the pressure increases (think about your cheeks when you try to blow through that tiny straw). In a way, you can say that the afterload of the left atrium is very high due to this mitral stenosis.
Source: MedLine Plus
This ballooning is going to cause complications…that we’ll talk about in a bit.
But because that left atrium can’t just get buff to handle those pressures, what you will start to see is the ballooning of that LA and then eventually the LA can’t handle those pressures and so that pressure increase will start backing up into the pulmonary vasculature. This will eventually cause pulmonary hypertension in these patients.
Source: Pinterest
But your pulmonary vasculature also isn’t meant to withstand high pressures either. Keep in mind that when your LV contracts it generates approximately 120 mm Hg of pressure in your body, give or take. Meanwhile a pulmonary artery pressure of greater than 25 mm Hg is considered pulmonary hypertension.
So, as you might expect, this build up of pressure continues to back up, until we get to the right ventricle. Can ventricles withstand higher pressures? They can. But just like the left ventricle in aortic stenosis, in mitral stenosis what you will get overtime is a hypertrophying and expanding of that right ventricle. So this is how, if left unchecked, mitral valve stenosis can lead to right sided heart failure.
What kinds of patients get mitral stenosis?
Unlike aortic stenosis which is generally more common, especially in the older population, mitral stenosis is often caused by rheumatic heart disease. Ok what is that though?
I don’t know about you, but when I was a kid, I feel like I was sick all the time, and that commonly involved either my ear or throat hurting.
And lo and behold, I feel like everytime I went to the pediatrician, the first thing they did was take that godforsaken SWAB and shove it down my throat and make me gag horribly.
What they were testing for, and what pediatricians have a very low threshold to test for (and rightfully so), is strep throat. But why so aggressive on the testing?
As it turns out, Group A Streptococcus infections are no freaking joke. If left untreated, even for just a couple of weeks, they can cause something called rheumatic fever.
Rheumatic fever, although triggered by a strep infection, is not a bacterial infection but rather a misregulated response of the immune system as a result. During this response, the immune system can attack specific tissues in the body, most commonly the joints, brain, and also – you guessed it – the heart. The immune system can target the heart valves – in this case the mitral valve – and cause inflammation and damage to it, causing thickening of the leaflet (aka stenosis).
Though the incidence of rheumatic fever is very low in countries like the US, this is why strep throat is so commonly tested for – I have personally seen older patients who had their mitral valve replaced and underwent open heart surgery as early as 16 years old because of rheumatic fever complications. However, in many patients, there is a slow immune response to the initial infection, so stenosis can sometimes still take quite a few years.
Why does left atrial ballooning matter in patients with mitral stenosis?
As I alluded to above, the left atrial ballooning we see with mitral stenosis can cause a big complication in a lot of patients, independent of heart failure.
Can you guess what it might be? Keep in mind we are talking about the left atrium, and in this case, we are going to see stretching and mucking around with that left atrial tissue.
That tissue is going to get irritated and pissed off.
And as a result, patients with moderate-severemitral stenosis commonly develop atrial fibrillation. As that left atrial tissue balloons out, stretches, and undergoes this structural shift, a bunch of ectopic points of conduction can form in that LA and – *voila* – you got yourself afib.
But this ain’t your typical rodeo AF… this is a *special* type of AF known as valvular afib. Depending on who you ask (Europeans, I’m lookin’ at you) – this term is a little passé but it is still used in the latest rendition of the American guidelines.
Valvular AF is a special beast, and is currently defined per the American guidelines as AFib in the presence of mechanical heart valves AND/OR moderate to severe mitral stenosis.
Why must we categorize this separately? It all has to due to risk of thrombosis in these patients. Whereas your typical CHADS2VASC (in NVAF) score of….4….gives you an average yearly risk of stroke of ~4.8%, patients with valvular AF have a much much higher risk of systemic embolism – and I’m talking a whopping 20-30% per year! It’s important to recognize the presence of these things when assessing a newly diagnosed AF patient because as you may recall from our AF OAC talk, these patients need to only be managed on warfarin, and NOT DOACs.
To me, it kinda makes sense that AF in mitral stenosis would cause a high risk of clot. Afterall, the main reason clot forms in AF to begin with is due to stasis, and that LA quivering. Now imagine having that AND having that blood struggling to move out of that LA and through the the LV. The limit of stasis does not exist.
Symptoms
Just like we see in AS, the first symptoms in mild mitral stenosis can be seen on exertion, and are actually symptoms that can mimic left sided heart failure, without any actual left ventricular damage/failure happening. As these patients progress and develop AF, the AF just makes it just that much harder for blood to flow through that mitral valve, now without even that “atrial kick” to support flow through. If progressed to right sided heart failure, patients will get the typical symptoms seen with right sided heart failure and a backflow of pressure into the venous circulation such as edema, fatigue, abdominal distension and ascites.
[Insert brain break here]
Aortic Regurgitation aka Insufficiency
Now let’s move on to valve insufficiency aka regurgitation. Remember that in these scenarios, we are basically dealing with “leaky” valves – valves that do not seal well and do not do their job at preventing backflow.
What kind of patients get aortic regurg?
Let’s start with aortic regurgitation. Again: location, location, location. The aortic valve sits between the LV and the aorta. Like aortic stenosis, patients can develop aortic regurgitation with things such as advanced age (aka the valve degenerates as your patient gets older and older) or also in patients born with congenital valve issues (aka born with the wrong # of leaflets). Things like infections of that valve (e.g. endocarditis) can also break it down causing improper closing. Hopefully it makes sense that patients that have dilated aortic roots can also get these leaky aortic valves. This can happen in patients with chronic hypertension or in patients with connective tissue issues, such as patients with Marfan’s.
Source: Children’s Health
pathophys of aortic regurg
Ok so we’re going to Magic school bus this now.
Imagine you are in that LV and with every squeeze and spitting out of 1 stroke volume of that LV, you get a bunch of that blood back in because of a leaky valve.
What’s going to happen in that LV?
Well, more and more blood is going to start accumulating in that LV, right? This is what we fancily call increasing end diastolic volume – quite literally, the amount of blood that the LV will hold at the end of relaxation will keep increasing.
Your LV wants to be a team player. It really does. In order to adapt, your LV allows itself to be somewhat more pliable/flexible so it can continue to accept higher and higher volumes so it doesn’t have to increase the amount of pressure in there.
As this progresses, your LV has to start pumping out more and more volume in order to make sure your body/aorta is getting enough blood in there to supply the body with oxygen – in other words, it has to squeeze more and more blood out and increase stroke volume in order to ensure enough forward flow.
However, if you remember our basics hemodynamics talk – what happens to pressure as volume increases? Think back to our hose analogy. Does the hose shoot the water further as you increase the amount of water flowing through the spout?
You bet it does. Because of these high volumes into the aorta, the aorta starts getting chronically high pressures. Because of these high aortic pressures, your struggling heart now has to pump against a high afterload that it ironically created.
If continued to be left unchecked, all this volume your LV has to handle along with this high afterload will cause pretty severe hypertrophy and structural changes of that LV, and eventually these patients will get these really round ventricles and have more contractility as they develop heart failure.
Symptoms of aortic regurg
Just like some of our other valvular issues, the symptoms of aortic regurg are slow to happen. This is all because our LV is able to compensate, and can expand a large amount to deal with the extra volume and is also pretty resilient against the initial high afterloads. When they do develop symptoms, they are very typical of left sided heart failure and can also experience angina or chest pain, because of their heart trying to work hard managing that high volume and afterload.
Mitral Regurgitation/Insufficiency
What kind of patients get mitral regurgitation?
One of the most common etiologies/causes of mitral regurgitation is due to something called mitral valve prolapse. This is when either the chordae supporting the leaflets or the leaflets themselves get all “floppy” and cause the valve to incompletely close.
It can also be caused from patients with messed up papillary muscles as a result from coronary artery disease – in other words, if your heart gets a decrease in blood flow to the area supporting these muscles, some of this muscle tissue can die, and it will no longer be effective in getting a tight seal. Another reason patients get get mitral regurg is simply from the stretching of that left ventricle in patients with things like volume overload (this is called functional mitral regurg).
pathophys of mitral regurg
OK so you got a leaky mitral valve. Again – know your location.
The mitral valve sits between the left atrium and the left ventricle. Think about being the blood within that LV.
You have two routes to go – you can either be pushed out to the aorta, which carries a decently high pressure associated with it (~80 mm Hg), OR you can flow back into the fairly low pressured left atria through a leaky valve. Just like many of us do in life, blood also wants to take the path of least resistance.
The “afterload” associated with that very compliant left atrium is wayyyyyy lower and easier to get through to than the normal forward flow into the aorta.
So your left ventricle is going to squeeze, and a good chunk of that blood is going to go backwards through that leaky valve into the left atrium. Because the left atrium has to deal with this higher volume and because the left ventricle is losing a lot of blood backwards, both your left atrium and the left ventricle have to accommodate a higher filling volume (aka preload) in order to make sure the net result is still adequate forward flow.
Let’s say that in different words. Let’s say when your LV squeezes, it loses 40% of its stroke volume to the left atria; the other 60% goes to the body. So – unrealistic values – but let’s say an adequate stroke volume for you is 10 mLs – the body will only get 6 mLs per beat instead of the 10 mLs it needs thanks to this regurg.
If your preload stays fixed, then 60% of normal stroke volume that should be 100% ain’t going to cut it. So the only way to fix this is to increase the amount of volume that these chambers are dealing with. So now let’s say you have more volume and your SV is actually 16 mLs instead of 10 mLs. You’ll still have the same issue – 40% of that will be lost to the left atrium – but because you are dealing with a large volume, the 60% that your body will receive will now be 10 mLs.
Still with me?
As that mitral regurg gets worse and worse, and the valve more and more leaky, severe mitral regurg occurs when more than half (>50%) of that stroke volume is lost the the left atrium.
In order to compensate, it should hopefully make sense that the left ventricle actually has to double its output. Because again – if you need that 10 mLs of stroke volume and you are using 50% per contraction – in order to compensate that LV will start having to spit out 20 mLs of stroke volume to ensure 10 mLs gets out to the body.
This is…..rough on that poor LV. What you end up with is crazy dilation of both that LV and left atrium, as well as hypertrophy of that LV since not only does it have to get all dilated to support the new volume, but it has to work harder than normal to contract double of its typical stroke volume out.
The heart is able to compensate for a long time – but eventually, something’s got to give. There comes a point where that super dilated, very stretched out and thickened left ventricle cannot compensate anymore.
The ironic part about these patients is even though they can have both systolic and diastolic issues, their EFs often stay “normal” because of the increased end diastolic volumes.
symptoms
Just like our other diseases, because your LV is technically able to get more volume and contract harder, especially in the beginning, patients may not have any symptoms, even on exertion – since after all, their cardiac output shouldn’t really change since their stroke volumes aren’t changing (remember CO = HR x SV). However, if they eventually tip over, their symptoms will be very similar to that of left sided heart failure.
Interesting but sad real life exampleof how valvular disease can be deadly:
The above little majestic creature was my childhood dog named Lucy. Now when we adopted Lucy, at her first vet appointment, we were told she had a heart murmur. Vet didn’t make it seem like a huge deal (and granted we weren’t the best with taking her to the vet every year). Lucy was totally fine, until at the age of 8 she started coughing one day.
It wasn’t an every second type of cough, but here and there she would start having a wet cough. We took her to the doctor and they got a chest xray on her.
And lo and behold they saw a really really big heart, a ton of pulmonary edema – in short, that valvular disease that Lucy probably had since she was a puppy finally caught up to her, and she could no longer compensate – she had developed heart failure.
She was still completely “normal” with the exception of the cough – we took her in for an ECHO before they would start therapy on her, and unfortunately the stress of the ECHO and being around all these people tipped her over, and she had florid ADHF and had to be put to sleep that same day.
I, of course, didn’t know about any of this stuff as a teen, and learning it over the years has really made me understand what was going on with our little Luc all those years ago, and really hits home to me why valvular disease is such a big deal and needs to be treated.
Thanks for hanging today – I know this was a dense one. Stay tuned for part 2 where we will be discussing valve replacement options and pharmacotherapy for these different patients!
Today we are going to be talking about some general stats stuff. For all my stats posts, I will always preface with the understanding that YA GIRL is NOT a statistician. At all. Seriously. I envy the brilliance of those people every time that time comes around during research.
With that being said though, I had no idea what was happening in stats when I was in school. To be honest, I didn’t really understand a lot of drug lit stuff until the tail end of PGY2 year but really when I finally had some time to sit down with this stuff and be like wtf am I actually looking at here and what does it mean?
Actual footage of me in school when stats came up. Source: GIPHY
Today we are going to have a lil talk on internal validity, external validity, and run-in periods. These are all fancy terms that I didn’t really get at the time but hopefully you might understand them a little bit better after this post.
✨✨✨These topics today are all things you should consider when reading/interpreting/presenting a journal club.✨✨✨
Happy holidays ya filthy animals. Love, me Source: GIPHY
Without further ado:
Running a trial and what to do with the data
Let’s rewind back to school-version me.
I used to think that trials were like super medical and very factual and very black and white. I didn’t realize understand that there’s about a million different ways to look at, and present, the same amount of data. When I did a journal club, I was like a lil parrot reciting everything that the trial did, and what they found. And I had no idea what it really meant.
This is my ploy to make you smarter than school-version of me. Do better than school version of me.
Ok: Let’s start with two ways to assess data. There’s two major ways to slice up your data and to analyze it. You can either use an intention-to-treat analysis or you can use a per-protocol analysis.
Source: GIPHY
Intention to Treat (ITT)
Luckily for us, even though these names are kinda fancy-sounding, they still make sense if you think about what they are saying.
In intention to treat analysis, you start off by separating and randomizing patients into your groups like normal.
Let’s say we are assessing two drugs against each other: Drug A versus Drug B. (original, ikr)
We’re about to start the trial.
Let’s say you get assigned to take drug A and I get assigned to take drug B. Now, you guys know by now I’m visual, so figured I’d make a graphic to illustrate this clearer.
We’re in our groups – let’s say the trial goes on for a total of 3 months, and then the data is pooled and looked at.
Intention to treat is exactly what it sounds like. As an investigator, I intended for you to be in the drug A group and I intended for me to be in the Drug B group.
So – no matter what happensafter that initial assignment – your data will be included with the Drug A group, and mine will go with the Drug B group.
👏👏👏Let 👏 that 👏 sink 👏 in 👏👏👏
Let’s put this in other words. Even if you skipped a bunch of drug A doses, or never took drug A OR ended up saying screw that and took drug B instead ….. your results will still be grouped with Drug A.
U might be like….. Source: GIPHY
Now, you might be asking yourself – why the heck would a trial do this?
There’s a couple of good reasons. By allowing patients to kinda do what they like, you are better mimicking what will happen in the real world.
Source: GIPHY
Are humans perfect IRL? Def not.
Real world really does mean that your patient might skip a dose, and not perfectly take your drug. But….. because of this loosey goosey allowances, you aren’t capturing the 100% true effect of thedrug, since not everyone is taking it exactly as they should be prescribed.
Source: GIPHY
We have these terms in lit called internal validity and external validity. The way I remember what they mean is I always think of internal validity as living within a bubble of a trial. And visa versa, external validity is outside of this utopian trial world – aka what happens IRL.
The real seinfeld fans will understand this bubble reference. Source: GIPHY
What do you think ITT analyses would have? High internal or high external validity?
Well, because we are kinda allowing patients to do what they would normally do, ITT trials have higher external validity because they better mimic real life.
The benefits of ITT
You might be asking yourself – I still don’t really get why someone would do ITT – and I think it can be best solidified by an example.
Let’s say you have a drug to treat hypertension and let’s say it’s FANTASTIC. It is really quite effective. Bravo. This is amazing, we did it! We saved the world of resistant HTN.
Eh, well. Not so fast.
Well…..let’s say this drug actually frequently causes explosive diarrhea. Like…. in a lot of patients.
Source: GIPHY
If you only conducted a per-protocol trial (which we will discuss soon), you will see ALL the benefits of how effective this drug is at lowering BP, but really not see some of the true effects of the drug IRL – which is – in reality, that not many patients will take it and many discontinue it on their own.
ITT can still capture these patients.
What to look for with ITT?
Kinda like I hinted above, whenever you have a ITT trial, you should always check out if they report things like crossover rate or discontinuation rate.
This could totally skew how you regard your results. Classic example I like to use is the AFFIRM Trial.
I just wanted to put this in because I think this is the cutest thing. Source: GIPHY
The AFFIRM trial was a 2002 study that looked at what the heck was better for treating patients with a fib – rate or rhythm control? This was an age old question and it was time to finally get the answers.
If you first glance at the trial, you’ll find that in these patients, there was no survival benefit found between rate or rhythm control – aka they were both equal – but you did see the rhythm control group trend towards increased mortality (that means it was a numerical difference but no stat significant difference).
It’s easy to look at this trial, read the results, call it a day, and go binge Wednesday on Netflix. But if you look into the analysis of the trial, you will see that it was a intention-to-treat analysis.
Low key love the OG wednesday for representing us fellow 5-headers proudly. Source: GIPHY
Next, if you check out how many patients crossed over (aka switched from rate to rhythm or switched from rhythm to rate), you’ll see that there was a statistically significantly higher rate of crossover in the rhythm control group with a WHOPPING 37.5% crossing over. In other words, almost 40% of patients that were analyzed as being in the “rhythm control” arm were actually taking rate control agents instead.
All of a sudden the results aren’t so black and white, huh? Kinda hard to really be able to compare these drugs for sure, knowing that more than a third of my patients assigned to rhythm control really ended up taking rate control agents.
What this does tell us? Well I think a few things. Rhythm control drugs are likely much less tolerated (which we do see in practice). This is really shown in this trial.
But if you really ask me based on this trial if both strategies are similar? Well, I would say this data is not convincing due to the extremely high rate of crossover. This would be a big con of the trial when presenting these conclusions (imo, of course).
Source: GIPHY
Per Protocol
Next up we have per protocol analysis. And – once again – it’s exactly what it kinda sounds like. I’m makin’ my trial, coming up with a protocol that you need to follow, and guess what – if you don’t follow it – even if you miss one or two doses – you are OUT – aka we are not including you at all in our data.
IT’S MY TRIAL AND MY RULES OK.
So back to our example – you’re allocated to Drug A, me to Drug B – if we’re using per protocol analysis, we will only be included in the data if you stuck to the script and took drug A and I only took drug B. Aka stuck to our assigned groups.
Knowing the above – would PP analysis have high external validity or high internal validity?
It would have high internal validity. Afterall you are in that perfectly scripted, take-every-dose, utopian trial bubble. This is good because it really tells you the true effect of the drug, On the other hand though, it might not really capture the true tolerance of the drug or the effects it would have in a “real world population”.
What to look for with Per Protocol?
Whenever you see that a trial conducted a per protocol analysis, check out if they report how many patients ended up being excluded from data and why. Good trials will list out example what percentage of patients were excluded, and great trials will tell you for what reason. This can help provide insight about the tolerability of the drug and other effects it might have.
Everyone in the OG colchicine trials. Titrate to diarrhea. Source: GIPHY
Modified Intention to Treat
Another thing to note (and again, not something I realized when I was in school) is that trials can do whatever the heck they want as long as they explain/report/define what they’re doing.
Because of this, trials can totally decide to analyze data based on a modified intention to treat, or mITT. What does that mean?
Literally anything! The investigators generally get to choose how they define this.
The can define it, for example, as “we will include you as long as you received the correct drug for the first “X” number of days”.
Whenever you see an mITT, make sure you understand how it is defined and how that might change interpretation of results.
Run-In Periods
Ah yes. Another term I threw around in school knowingly but had no clue. Let’s talk about what a run-in period actually is.
Source: GIPHY
A run in period is a period of time between the actual recruitment of the trial to when the trial actually starts where all participants get the same treatment.
The data you are trying to capture in your trial (for example, mortality difference) isn’t actually being recorded during the run-in period. This is like a pre-trial period.
Hopefully the graphic I made above kinda illustrates it better. If you were to do a trial, first you have to get a group of people who are going to participate in the trial. Then you put them through an investigator defined “run-in” phase. During this phase, the data that is being collected/what happens to these patients is not included in the results of the actual trial.
During the run-in phase, you are going to have a certain number of patients drop out for various reasons. Once this phase is over, now you can finally start the trial. You will take all these remaining patients, randomized them into different groups (e.g. Drug A vs Drug B) and now the data for the trial will start being collected for the results.
Why do a “run-in” period?
There’s quite a lot of reasons a trial might decide to incorporate a run-in period, some sneakier than others.
A common reason for a run-in period is using it as a sort of “washout period”. For example, hypothetically let’s say we wanted to see the true effect of an anti-HTN medication. Well a ton of patients in that trial might already be on all different kinds of doses of all different kind of anti-HTN drugs, so in order to make sure the effect is from the drug itself and not a residual effect from another drug, you could incorporate a run-in period to ensure that all patients are starting at a true “baseline”.
Or let’s say they might be on other drugs that interact with the drug you are testing. Classic example is patients on an ACE-I – they need a 36 hour period of washout prior to starting an ARNI due to risks of angioedema and whatnot. A run-in period might require that everyone who was previously on an ACE-I stop these drugs so they can safely start the trial.
Source: GIPHY
A trickier kind of run-in period is one that can be for “safety and tolerability”.
You might be asking – what’s tricky about that?
Well, your results and your interpretation of said results might become skewed. Let’s say we are trying to give patients a new drug, and we have a run-in period where we declare that in order to be randomized/start the trial, all patients must be able to tolerate a drug at a certain dose. Oftentimes they will have an uptitration scheme (e.g. week 1 of run-in period you get 5mg, week 2 10 mg, etc).
And along the way, a bunch of patients are having to drop out, because they don’t tolerate the drug they’ve been getting or have unacceptable side effects.
These patients aren’t being represented in the results of that trial. So in other words, often “run-in” periods can be a sly way for investigators to get a cream-of-the-crop, hearty, more likely tolerate/have less side effects patients when they are starting their actual trial. Because of this, noted “side effects” or ADRs or discontinuation rates may be a lot more common in practice compared to life within this trial.
Source: GIPHY
Putting it into Practice with an example!
I’m a very hands-on learner. Can’t just sit there and read all day. Let’s test your knowledge with a real life example.
We are going to discuss the PARADIGM-HF trial. This is the landmark trial that got sacubitril/valsartan (aka Entresto) FDA-approved for the treatment of patients with systolic HF (HFrEF).
I want you to skim over this trial. What kind of analysis was there? What does this tell you? Did they have a run in period? How might this skew results? What might analyzing this trial tell you about real-world use of Entresto?
Source: GIPHY
I’m serious.
Seriously, go check out the trial!
Answers below (! spoiler alert)!
Source: GIPHY
What kind of analysis did they use? They used an intention to treat analysis. This means that the trial has the potential to have more real-world applicability.
Because I see the term “ITT”, I’m going to see if they reported crossover rates.Don’t see this reported, but they do report that 17-20% of patients discontinued the drug during the trial which is interesting. The good news is, this # was decently similar between groups so should balance out.
Did they have a run in period?
Yep, looks like they did. In order to start the trial, you had to complete a run-in period. They report it as a single-blind run in period, where all patients had to receive and tolerate enalapril 10 mg PO BID x2 weeks then the ARNI at 100 mg PO BID then 200 mg PO BID for 4-6 weeks.
All patients with significant side effects did not continue onto the trial.
Couple of things to unpack here.
School-version me would be like OK cool this is what they did.
But what does this actually mean, clinically?
Source: GIPHY
To understand that better, first we should assess – are they high doses? Low doses? What?
Well, these are pretty hefty doses of drug. Starting dose of enalapril is 2.5 mg PO BID, and 10 mg PO BID is really a full, basically target dose of this drug. Then these patients had to tolerate high doses of the test drug too in order to be randomized.
Next you should consider what “side effects” patients might have experienced on an ARNI or ACE-I. Immediately things like hypotension, hyperkalemia, dizziness, AKI come to mind.
Now, the PARADIGM HF is a robust trial, so they did good work and made sure to report out how many patients were kicked out during run-in and for what reason. What you end up seeing is 19.8% of patients that were supposed to be in this trial were excluded from participating because of things like adverse effects, lab abnormalities, etc.
Source: GIPHY
So even before this trial is even STARTING, we are kicking out 1/5th of patients and screened them out because they aren’t able to tolerate these drugs.
Now, what is that going to do to your interpretation of results? Well, we already know that the patients we are going to end up randomizing/looking at for data are already these more robust, more “cream-of-the-crop” variety who are less likely to experience hypotension, less likely to experience hyperkalemia, etc.
And when we end up looking at the results from these patients who actually ended up in the trial, we still see significantly more hypotension, AKI, cough and hyperkalemia in the sacubitril/valsartan arm.
What this trial really tells me – is that even despite an intention to treat analysis, the presence of this run-in period in this trial really skews the type of “real world” patients that I might see in practice.
It also means that – heck yeah – sacubitril/valsartan really does cause hypotension and other things in practice, and I can probably expect to see even more of these ADRs in real life because of the way this trial was conducted.
(Side note – GDMT is very important in our HF patients and it’s important to get ARNIs on board for those who can tolerate it! This is not to say ARNIs are not an integral and important part of the GDMT bucket. I’m a big believer in ARNIs (….for HFrEF but that’s another story for another day).
So, how’d you do?
Hopefully today you understood these terms a little bit better, and can move on by incorporating these ideas, these analyses, more and more in your journal clubs so you start to get a more robust idea of what the trial actually means and what the data is actually telling you, rather than just reciting what happened in the trial and what was concluded.
Happy Holidays to all!
Source: GIPHY
On a personal note, this was my first year coordinating/teaching core cardiology lectures for students at my institution. Shout out to each and every one of them for sticking with me through all 8 hours of lecture!They the real MVPs.
Happy September everyone! As a northeast coaster, I am definitely looking forward to this fall and the cooler weather. I am indeed a basic bitch when it comes to the autumn (guilty as charged). I have been living for my morning pumpkin cream cold brew.
It’s literally me. Source: Jacobgraye.com
Today is part 2 of our VTE series which will focus on the presentation and diagnosis of DVT and PE.
If you haven’t checked out part 1, I would definitely recommend giving that a once-over before reading today’s post.
Alright, without further ado, let’s get into it!
Ratatouille 4ever. Am I the only one who thinks rats are cute? I had a pet rat for a bit growing up – we found it drowning in a barrel of water outside after rain and took it in. My dad made me let him go in a field. Prob for the best. Oh, and source: Tenor
Part 1: Deep Vein Thrombosis (DVT)
Presentation
So, from part 1, we already know that a DVT is when a clot (aka thrombus) forms in the vasculature of the deep veins.
Source: TheSun
When a patient presents with a DVT, they commonly report some hallmark symptoms. These include pain, swelling, and redness at the site.
Well, – we already talked about heart failure, and you also said lower extremity swelling is a hallmark symptom of that – so, how can I tell if it’s a DVT or just run-of-the-mill stable heart failure?
The biggest differentiator is whether the swelling unilateral (occurring on only one side) or if it is bilateral (happening on both sides).
The chances that your patient has an acute clot/DVT in both their lower extremities at the same time is very low (but not impossible).
Generally, DVT s/sxs (signs and symptoms) occur unilaterally, whereas heart failure swelling is bilateral. You can check out the differences between a patient’s legs with an acute DVT in the pic below – you can see the classic swelling and redness immediately.
Acute DVT. Source: Wikipedia
👏Location, 👏Location, 👏Location
Just like the most important rule of real estate, location is also important to consider when treating a DVT (or should I say, deciding whether or not to treat a DVT – but we will get there eventually).
Source: GetYarn.Io
I am getting seriously bad flashbacks from the long journey of buying my first house about a year ago in this market in NJ *shudders*.
The majority of DVTs occur in the lower extremities….and when I say the majority, I really mean the majority.
Upper extremity DVTs are rarer, and most of them are actually due to iatrogenic (meaning we caused them as healthcare providers) reasons. With that being said, a lot of upper extremity DVTs happen in the hospital.
Source: GIPHY
Can you think about why a patient in the hospital might get an upper extremity DVT?
Source: GIPHY
It’s because we’re sticking so much stuff into em! Any IV line, cath, etc is a potential site for a VTE to happen. That’s because not only are we breaking open part of the vessel during insertion (aka triggering that extrinsic coag cascade) but we also have a foreign object in the vessel (cue the intrinsic coag cascade). Both have the potential to trigger the clotting process.
Source: Nurse Your Own Way
An ✨essential✨ thing to assess when you’re discussing a DVT event is where the heck the clot occured.
We have a bunch of veins, but not all of them are equally “important”.
I’ve also been watching the RHOA. Sry not sry. Source: Tenor
In fact, we don’t even really need all of our veins. If you remember in our ACS talk, we discussed what happens in CABG or coronary artery bypass grafting. The surgeon will actually remove (the proper word for this is HARVEST but idk why but that literally gives me a lil of the heebie jeebies) a vein from the leg to use as a new vessel to connect in the heart/aorta.
Source: ResearchGate
Additionally, not every vein has the same risk of a clot lodged there to embolize and go to the lungs. This is a big factor that is going to drive differences in treatments (or lack thereof).
As we discussed in our previous post, a big complication of DVTs is that a part (if not all) of that clot breaking off in that vein, traveling up through our inferior vena cava, into that right heart, out of the RV and *pop* right into that pulmonary vasculature. And thus, DVT -> PE.
Source: MakeAGif
Source: GetYarn.com
Rule of thumb: as the name would suggest, we are talking about the deep veins here. DVTs are the clots that carry that high risk of embolization.
In our body we also have what is called “superficial” veins (they’re so vain….get it?!). These are smaller and have less chance of embolizing. In fact, if a clot forms in a superficial vein, often the risk of anticoagulation does not outweigh the benefit of treating that clot. We will dive into this more later during our treatment talk.
There’s also a breakdown between what we call proximal DVTs and distal DVTs.
Distal deep veins are found in the calves and include the anterior tibial, posterior tibial, and peroneal vein.
The proximal veins include the external iliac, deep femoral, and popliteal veins.
Proximal DVTs (aka the ones closer to the trunk of the body – aka the ones in your thighs versus the ones in your calves) tend to be more clinically important because they are more commonly associated with embolizing/breaking off and taking the fast lane to the lungs where they can cause a pulmonary embolism.
Source: CodeBlueMemes
This doesn’t mean that we don’t treat distal DVTs. Distal DVTs should be treated if any of the following is met:
your patient has symptoms
if the DVT has grown/extended
if there is high risk for extension of the clot (e.g. high d-dimer >500, prolonged immobility, extensive thrombosis in multiple veins, unprovoked DVT, prior hx of clots, etc)
If you happen to find a distal DVT by chance (aka your patient had no symptoms and no risk factors for extension), you can actually hold off treating that bad boi and should just get serial imaging (1 image q week) for 2 weeks. As long as that bad boi doesn’t extend on serial imaging over time, no anticoagulation is the way to go. However, if it starts to extend, especially into the proximal veins, that lil’ DVT just bought a ticket for AC.
Superficial Vein Thrombosis (SVT)
You also have a series of blood vessels in your body known as superficial veins. SVTs generally affect the lower limbs, with about 2/3rds of lower-limb SVTs occuring in the saphenous vein. It is not uncommon to find a SVTs at the same time as a DVT – they often can occur together.
Source: CoreEM
Every time you have a patient develop a new clot, I’d recommend actually reading out the report and seeing in which vessel did this clot occur. If it’s exclusively in a superficial vein, most of the time, we’re going to d/c that anticoagulation unless they are at increased risk of clot progression to DVT or PE.
This intervention is simple but may prevent patients from being on anticoagulation where its not needed.
Source: Redbubble
At the end of the day, the decision to tx (or not to tx) is really dependent on risk versus benefit. We will go into more details in the treatment section.
Diagnosis of DVT
There’s a bunch of different components involved to diagnose a DVT. Patients present with all kinds of symptoms all the time, like lower extremity swelling – does that mean we should get tests and run imaging on every patient that presents with lower extremity swelling?
Probably not (and by probably I mean definitely). That would not only cost the healthcare system a ton of money, but also a ton of time. And then those machines also wouldn’t be as available for people that really need it.
Source: GIPHY
So how do we figure out who to test and who to not test?
For this, we use a ‘scoring system‘ which basically gives you an idea of their “pretest probability” that they are having an active clot.
One scoring system that is commonly used is called the Wells’ criteria. The Wells’ criteria takes a bunch of risk factors into account and spits out what your patient’s likelihood of having a DVT is. You can check it out below:
Source: MDCalc
If the score is low enough, your patient has a low probability, and other etiologies should be considered. But if it’s high enough, you’ll want to pursue a potential DVT diagnosis.
Source: GIPHY
What about some labs? There is a lab, known as D-dimer that we can test for. But what is d-dimer?
D-dimer is a degradation product of cross linked fibrin and also a marker of inflammation. Keep in mind that your body has mechanisms to break down an existing clot, just like it has mechanisms to form a clot. If you have a clot, your body is able to naturally break down existing clot, break down that fibrin, and increase d-dimer levels as a result.
When you think about it, we are really relying on your body’s natural ability to break down an existing clot in medicine very often. Every time you give anticoagulation to a patient with a clot, keep in mind you are doing nothing to existing clot. You’re just preventing more clot from forming. Giving anticoagulation really depends on your body’s ability to break down clot for treatment to work.
D-dimer is also…..imperfect.
Source: Tenor
A rule of thumb is that the d-dimer is good for ruling out DVTs (in other words, if your d-dimer is negative it is a good indicator that there might not be a clot) – but if your D-dimer is positive…. it does not always mean your patient has a clot. Many, many, many factors can contribute to high d-dimers outside of the VTE world (some include age, cancer, etc).
So now you have your d-dimer, your wells score. Everything is pointing to a possible VTE. These two by themselves are not enough to diagnose a DVT, they are more of screening devices we use to figure out who to actually test.
Next we get imaging to definitively diagnose. Methods include 🌟compression ultrasonography🌟 (aka a 🌟Doppler🌟) or venography.
What is a Doppler?
Ok, bear with me. Do you remember the term the “Doppler effect” somewhere in the far reaching corners of your brain? Like the part of your brain with the cobwebs that contain other stuff like knowing what the ancient Mesopotamians ate and did.
The doppler effect is the name of the phenomenon that occurs when a moving object producing sound moves by a stationary object.
The classic example of the doppler effect is an ambulance passing by. As the ambulance passes by, the frequency or pitch of the sirens changes from a constant high frequency to a constant low frequency, even though the technical frequency has remained the same.
Source: GIPHY
A Doppler ultrasound utilizes the same principle. The doppler ultrasound is a non-invasive imaging test that uses sound waves to detect blood flow in vessels. By spitting out sound waves that are reflected from moving objects (aka your red blood cells), a sonographer can detect interruptions in flow (aka clots). These bounced-off sound waves then are translated back into the computer to create an image. So, ultrasound indeed is ultra-sound. 🤯🤯🤯🤯
Source: GIPHY
Ultrasound is truly mind-blowing and magical when you find out how it works.
If you want to learn more about US and how it works, I highly recommend this layperson-friendly podcast episode from Stuff You Should Know (one of my favorite podcasts – besides true crime/murder ones).
Doppler US is awesome because it is: quick, painless, noninvasive (and magical as you’ll learn). Doppler is usually considered the 🌟gold standard🌟 imaging to diagnose a DVT because it is non-invasive and quick. However, in certain patients, such as morbidly obese patients, Doppler may not be effective at getting a clear picture.
What is venography?
Venography is a more invasive technique that involves injecting a radiopaque contrast dye (aka a colored dye that will appear during X-ray) into your vessels and then taking serial X-rays. The dye has to be injected via catheter (flexible tube) at a certain site depending on where the clot might be so the doc will typically assess through the femoral vein in the groin and snake the catheter to the appropriate location before injecting the dye. The dye will light up in your patient’s vessels like a Christmas tree to help visualize blood flow (or clots).
What venography looks like. Source: Thoracic Key
Part 2: Pulmonary Embolism
Presentation
Ok so you got a clot in your lower extremity veins, and a pesky little piece of that clot breaks off (aka embolized into your lungs). Not great.
Source: CFCH
We already talked in part 1 about how these patients can present very, very severely….I mean, they can even present in a code blue – I’m talking full on cardiac arrest. If you remember that’s due to their RV basically crushing their LV and getting overstrained.
So yes, these patients can present mid-CPR to the ED, or even unfortunately not make it to the ED.
I sincerely apologize but I am physically unable to mention CPR without remembering this scene from the Office because of who I am as a person. IYKYK. Source: Tenor
There are all kinds of PEs (as we will soon discuss), and some can present more milder than others. Common s/sxs include tachycardia (fast heart beat), dizziness, sweating, fever, sudden severe shortness of breath, leg pain/swelling (because often they have a concomitant DVT), and chest pain.
Patients can also have no symptoms at all. What a wild world. So you can either be asymptomatic or you can be dead.
Categories
PEs are broadly broken down into 3 categories based on severity: massive, submassive, and nonmassive.
How I feel about this naming system. Source: GIPHY
Listen, I didn’t name these categories but I low-key hate how they sound together.The massive and submassive is ok, but idk why but I hate the nonmassive part.It’s the worst when I’m teaching new students and they all sound alike.
Let’s start with the worst kind: massive.
The major defining feature of a massive PE is systemic hypotension. Although hemodynamically unstable PE is often caused by large clots, the hallmark is the hypotension, and so the term “massive” PE doesn’t necessarily have to do with the size of the clot, but rather with the hemodynamic effects it causes.
As we talked about in part 1, this causes severe cardiopulmonary failure because that RV gets overloaded, pushes on that LV (aka septal bowing happens) and bam – decrease in cardiac output and since BP = CO x SVR -> systemic hypotension.
As you might have figured, this condition has the highest mortality rate (and the mortality is pretty high – anywhere from 25% to a whopping 65%).
These patients will have sustained hypotension (aka <90 mm Hg systolic or a drop in systolic arterial pressure of at least 40 mm Hg) for >15 min. RV strain can be seen on ECHO like in the pic below:
Look at that lil squished LV! Source: annemergmed
A submassive PE is when your patient is still hemodynamically stable, but are already showing some RV dysfunction or hypokinesis (not contracting as hard/moving as well as it should).
A nonmassive PE is the friendliest of all PEs. Your patient does not have any evidence of RV dysfunction on ECHO and are hemodynamically stable. These patients may have symptoms or may even be asymptomatic.
Source: GIPHY
You can also break down PEs based on their location. Going from the biggest -> smallest, you have saddle PEs, lobar PEs, segmental PEs, and subsegmental PEs.
Saddle PEs are oftentimes the most severe, since the clot gets lodged before your lung vasculature branches off (the fancy way is saying it occures at the bifurcation of the main pulmonary artery), thus blocks blood flow to both sides of the lungs.
Source: Healthline
Source: UpToDate
Diagnosis
The diagnosis of PE is somewhat similar to that of DVT in that you again start with a pretest probability scoring system. In other words – a lot of people present with shortness of breath – a lot of people present with chest pain. Are we going to test everyone for an acute PE? Yeah, no.
Just like our DVT diagnosis, PEs also have their own Wells Scoring System for patients with suspected PE in the ED. You can check it out below:
Source: MDCalc
Labs also include a d-dimer, and unlike DVTs, you can also get cardiac troponins (which we talked about in our ACS posts) – if the PE is bad enough, it will cause cardiac strain and you’ll get that troponin bump.
Unlike a Doppler, though, PE has its own type of imaging to assess.
These include ⭐ chest CT⭐ (aka computer tomographic pulmonary angiography – try to say that 5 times fast) and also ECHOs (like I alluded to above).
Chest CT is the ⭐ gold standard⭐ because it is more specific in that it is excellent at detecting insufficient filling and/or clot. Chest CT is so great these days, that incidental PEs are sometimes found (AKA you had a clot and didn’t even know and had no symptoms but we found it by accident).
A chest CT utilizes radiation and is an imaging modality that is able to take very very very thinly sliced pictures of the chest. Oftentimes patients will also get special contrast agents intravenously. This contrast dye will go into your chest vasculature and light up on the CT scans, making it even easier to see issues like clots.
A CT chest. Source: Vanderbilt.edu
Since we are talking some radiation – fun fact: Marie Curie was actually Polish not French as a lot of people suspect by her name. She was born Maria Skłodowska and not only termed the word radioactivity but also discovered two elements – radium and polonium (named after Poland, the place of her place of birth). Both Marie and her older daughter died of radiation exposure (her older daughter died at 58), but her younger daughter lived until 102!Both my parents are from Poland, so you better believe we visited her museum the last time I was there:
Source: MEEEE
Alright, alright now ECHOs – or echocardiogram. An ECHO can help you visualize more of the heart’s structure and function – and see how it moves. This is where you can detect septal bowing and RV strain. In fact, ECHO also uses ultrasound just like our dopplers do!
Lastly, not as common, but there is something called a VQ scan aka a ventilation (the V) – perfusion (the Q) scan. How does this work?
Think back to how your lungs work. Keep in mind that your lungs need both good perfusion and good ventilation to work.
In a health patient, air enters the lungs and going into our little tiny air sacs called alveoli. The alveoli puff up with good oxygen/air and are covered in capillaries. Our capillaries are able to take the oxygen and good stuff out of the alveoli and trade it for some bad stuff like carbon dioxide that we then breathe out.
Source: Verywell Health
In other words, you have to make sure your alveoli are nice and open and are able to take it good air/oxygen. If you have alveolar damage, an empyema (a cavity full of pus in your lungs), or other things going on, your alveoli will not be able to fill nicely with air. No matter how perfect your capillary blood flow to those alveoli is, it will still not be able to get good exchange because there is a problem with your alveoli/ventilation.
Visa versa – if you had great alveolar filling but terrible blood flow (aka bad perfusion) in those capillaries like…in a PE…you still won’t be able to get good exchange. In this case, your ventilation would look good but your perfusion would be crap.
This is what the VQ scan tests for. First your patient will breathe in some nice radioactive material (we call this a tracer) and X-rays will be taken. Next, they will inject a lil radioactive stuff into your patients vein and take an X-ray to detect blood flow.
In a healthy patient, there should be a “matching” good perfusion and ventilation. However, if patients have a PE, their perfusion will be decreased.
Source: Stritch.luc.edu
Thanks for hanging around today. Stick around for the next post on treatments! Until then, enjoy the fall season.
Today we’re gonna begin to tackle a core cardiology topic: venous thromboembolism 🎉🎉. For the purposes of today’s intro, we’re going to focus on defining VTE, understand the anatomy, and nail down some core pathophys concepts before we get into more specifics in our future posts.
But before we dive into everything – you know me – we’re going to break down exactly what these words mean.
Source: GIPHY
What is venous thromboembolism?
Let’s start with the basics: defining venous thromboembolism.
Venous, as the name suggests, pertains to the veins. For everyone who remembers our talk on basic anatomy/hemodynamics, veins are defined as vessels that carry blood back towards the heart. Most veins contain deoxygenated blood – but not all – the pulmonary vein is the exception to the rule – she carries oxygenated blood from the lungs back to the left side of the heart.
Source: Shutterstock
Thromboembolism is a combo of the words thrombus and embolism.
A thrombus is a fancy name for a blood clot.
A embolus is what happens when that blood clot (or a piece of that blood clot) breaks off and gets carried in the bloodstream and lodges itself in another area.
An embolism that just lodged itself somewhere new. Source: GIFTenor
What falls under the category of a VTE?
Thromboembolism is a blanket term consisting of two main subtypes: you got your deep vein thrombosis and you got your pulmonary embolism.
A deep vein thrombosis, more commonly referred to as a DVT is when a blood clot (aka thrombus) forms in one or more of the deep veins of the body (usually in the legs). Key idea here is veins – not arteries.
A pulmonary embolism, commonly referred to as a PE, is when that blood clot gets stuck in an artery of the lung and blocks blood flow to a part of the lung. The majority of pulmonary embolisms start off as DVTs in the leg; those clots then break off and travel to the heart where they lodge in the lungs.
Anyone else remember high school musical? My school made us perform those songs for our parents in 7th grade. *shudder*. Source: GIF Tenor
Why are DVTs and PEs considered VTEs but a stroke is not?
All of this goes back to basic anatomy, but I think it’s important to re-visit and re-remember so you can understand these concepts instead of memorize them.
Let’s revisit how blood flows in the body, starting with a vein in the legs. Let’s just pick a big one – the femoral vein.
Source: Wikipedia
Alright let’s say a clot forms in your femoral vein (sorry, tough luck). Check out the diagram of the femoral vein to get an idea of where this clot is forming.
If that clot breaks off, where is it headed next? Well, first off, we know that clot is headed back towards the heart (since it is a vein, by definition of the word).
That clot is going to travel through the femoral arteries, through the iliac veins, and enter the big kahuna of deoxygenated blood flow – the inferior vena cava.
I like to think of the inferior vena cava as the superhighway vein of the lower part of your body – the smaller veins of your lower body will all deposit their blood into the inferior vena cava, the vena cava will collect all this blood, and then superhighway it back up to the heart.
The inferior vena cava then connects directly to the right side of the heart, and, you guessed it, it’s still carrying that pesky little embolus along for the ride.
Source: Shutterstock
Once in the right atria, that clot is going to head through the tricuspid valve, through the right ventricle, and then go through the pulmonary artery into the lungs.
Now, remember that the pulmonary artery is going to break down into smaller and smaller vessels, eventually becoming teeny, tiny capillaries that wrap around each alveoli, and get oxygen.
Source: Verywell Health
In other words, in most patients, there’s absolutely no way a DVT is going to cause a stroke, since that DVT is going to embolize and get stuck either in the lungs or somewhere on the route before. If you remember, a stroke is an arterial-based clot, and usually comes from the left side of the heart, out the aorta, and up into the arteries that feed our brain.
Ok now time for a tangent 😈😈😈😈😈😈😈
Now, a little bit of extraneous information, but there is a way that DVT can cause strokes, and it all depends on your patient’s anatomy/structure of their heart.
Can you think of how the heck this would happen?
Well, I told you there’s no way that clot could pass through the lungs and get to the other side – to the left side of the heart – that sucker is going to get stuck in the lungs in those teeny tiny capillaries.
So how does this happen?
How does that clot go from the right side of their heart into the left side of their heart? The answer is simpler than you might think.
Source: GIPHY
This can happen when there’s a literalhole in between the right and left side of the heart.
You heard me. A hole.
Source: GIF TENOR
We call this hole a patent foramen ovale, or PFO.
Let’s back track a bit.
When we’re all lil guys in the womb, we need this hole (the foramen ovale) to bring blood from our right atria to our left atria – thus bypassing the lungs – since we’re aren’t USING our lungs in the womb – we get all of our oxygenation from our mother’s blood.
Source: Mayo Clinic
At birth, the foramen ovale is supposed to close up – but in about 25% of patients, it doesn’t completely close. In most patients, this isn’t an issue and nothing ever happens – in fact, YOU might have a patent foramen ovale right now reading this and you would never know.
Source: GIPHY
However, if patients with a PFO have a DVT, they can end up getting what we callparadoxical embolism – where that clot travels from the venous side to the arterial side (because it pops right from the right side of the heart directly to the left) – and end up getting either a stroke, or an arterial clot somewhere.
We might test for a PFO if you are otherwise a healthy person without any other risk factors for stroke (e.g. no afib, for example) and present with a new acute ischemic stroke.
Can you think of how we might test for the presence of a PFO?
It’s too hard/small to necessarily visualize the hole itself on an ECHO (an ultrasound of the heart) but if we add a little ✨spice✨ we can.
Let’s add some bubbles to the mix.
Source: GIFTenor
Bubbles? Yep, you heard me. This test is called a bubble study, aka a saline contrast study.
Unlike Grey’s Anatomy or whatever other show you might have watched, a little air injected into our veins is really not a big deal – it doesn’t actually kill your patient or cause immediate arrest like popular culture might have you believe.
In a bubble study, your physician will take a sterile sodium chloride solution and *shake shake shake shake shake* until little teeny bubbles form and it’s all frothed up. They’ll then inject this into a vein.
Now following our anatomy, that solution is going to end up either in the SVC or IVC and enter the right side of the heart.
While this is happening, the doc will do an ECHO at the same time. The ECHO will enable them to physically see the air bubbles.
Source: GFYCAT
If the doc sees the air bubbles enter the RA, then the RV, and then…disappear? We’re good. Those air bubbles all went through the pulmonary artery (PA) and were expelled through the alveoli.
However, if the air bubbles all of a sudden end up on the left side of the heart? You’ve likely got a PFO, my friend.
Source: GIF Tenor
I’ve always thought this test was so cool in its simplicity. A lot of medicine isn’t as “complex” as we might think it is – by using simple concepts, we can get some pretty powerful info out of it.
OK side tangent over.
Why are PEs dangerous? How can they kill you?
The last thing I want to introduce today is the concept of why a pulmonary embolism can kill your patient – and can do so pretty instantly. For those of you who are familiar with the advanced cardiac life support (ACLS) algorithm, you might remember that pulmonary embolism is one of the causes of asystole or pulseless electrical activity (PEA) in cardiac arrest.
Why does this happen? Do you just get deprived of oxygen because there’s a clot in your lungs and some of that blood can’t get enough O2? Did the clot block all of your blood flow?
So, it is possible for the clot to just be SO large that it traps itself and blocks off your pulmonary artery, preventing forward flow. This is rarer, but as you might believe, causes pretty instant death.
The main reason we see PEs being so dangerous are actually due to the effect that the clot has on the right side of the heart.
What effect do you think that clot in your lungs has on your right heart?
Well, let’s go back to the idea of simple physics and what happens when a fluid tries to go through a smaller space. What’s going to happen to the pressure before that blood clot?
As less blood is able to travel easily through the lungs, more blood is going to get “backed up” and the pressure of the structures PRIOR to the clot is going to INCREASE as a result.
If you think back to your simple anatomy, the RV sits prior to your pulmonary vasculature. As that clot blocks blood flow, the pressure in your RV is going to get higher…and higher…and higher.
Source GIPHY
Depending on how high the pressure is, your RV might still be able to push through that pressure. But if it gets increasingly higher, we will start seeing physical changes in your heart from this increase of pressure.
As that pressure increases, your RV is actually going to start growing and cause what we call “septal bowing”. This means that your RV is going to start pushing against your LV.
Your interventricular septum is the fancy name we call the tissue that separates your RV from your LV. Under normal circumstances, that septum shifts towards your RV, making your RV crescent shaped from above (e.g. if you were looking at a cross-slice of your ventricles).
Source: REBELEM
Now back to our PE patient – as that pressure builds up in the RV, that septum is going to start bowing (leaning) the other way, crushing the LV.
Source: CHEST
As that RV continues to deal with higher and higher pressure, it will eventually be unable to squeeze against these high pressures AND the septal bowing may become so severe that it compresses your left ventricle stopping cardiac output.
This is why a PE can become so dangerous. The upstream effects that that clot can cause can be disastrous.
And that’s it for today’s discussion. Not leaving on the happiest note, but hope going through the anatomy and pathophys today was helpful before moving into more specifics like diagnosis, signs and symptoms, and of course – treatment.
Hey hey, today we’re going to start talking vasopressors – we’ll start with an overview of the background material and then delve into our first pressor we’ll discuss: phenylephrine.
Let’s get into it already!
What is a vasopressor?
Source: Cheezburger
Vasopressors, also commonly referred to as pressors, are a group of meds that contract (tighten) blood vessels and help to raise blood pressure.
The pressors we will be talking about in these series include:
Phenylephrine (discussing today)
Norepinephrine
Epinephrine
Dopamine
Vasopressin
How does blood pressure work?
I would recommend a quick refresher of blood pressure and hemodynamics here, but just a friendly reminder that blood pressure has two main factors that affect it: blood volume and diameter of blood vessels (controlled by squeezing and relaxing).
I like to use a garden hose as an analogy.
Let’s say you have a standard rubber garden hose – no attachment at the end – and that house is attached to the spout. Let’s say you nudge that spout and turn it a little bit.
Source: Charleston Crafted
What does the water at the end of the hose look like? Probably just dribbling out a little at the end right?
Source: Shutterstock
But what happens if you let more water go through that hose? In other words, what happens when you open up that spout more and let it go at full speed?
All this garden hose talk is making me want to go to the bathroom. Source: Shutterstock
More water, more pressure, and the further the water at the end of the hose will go.
Alright, alright: TLDR: our hose analogy has showed us that the more volume through the hose, the higher the pressure. The less volume the less pressure.
Now let’s say we leave that spout alone, keep it at a constant flow rate.
Source: GIF TENOR
So volume will remain the same in this scenario. Now let’s move to the end of that hose. It’s definitely spitting out some water, but that water isn’t really going too too far. Just kind of leaves the hose and makes an arc as that water falls down to the ground. Like this cute lil kid on the right.
Source: GFYCAT
But what happens if we start to mess with the amount of space we let that water squeeze through?
What happens if we put our hand at the end of the hose and block 80% of the opening at the end of that hose?
That water is going to shoot way, way further than it did before. By restricting the amount of space the water had to flow through, you effectively increased the pressure of the water moving through that hose.
Source: GIFTENOR
This is actually what garden hose attachments take advantage of. By forcing the water through a few tiny holes, the water that exists will have a much higher pressure and shoot much harder and go much farther. Who knew basic human hemodynamics was very similar to garden plumbing? (told ya cardiology is kinda cool).
The formula for blood pressure therefore includes fancily named variables representing blood volume and vessel size.
Blood Pressure = Cardiac Output x Systemic Vascular Resistance
aka
BP = CO x SVR
, where cardiac output represents circulating blood volume and SVR represents the squeeze of your blood vessels.
Cardiac output represents how much blood leaves the heart and goes to your body per unit of time. The formula for cardiac output is:
Cardiac Output = Stroke Volume x Heart Rate
, where stroke volume (SV) is the amount of blood the heart pumps out per beat. It’s important to incorporate bothstroke volume and heart rate into the formula for CO, since even if your patients has a great stroke volume – but let’s say their heart rate is really low in the 30s – their heart isn’t getting enough blood out to those tissues right?
Tying it Together
To increase our blood pressure, our vasopressors all work on at least one (if not both) factors (SVR or HR) within our blood pressure formula. Having a good understanding of the basics of the these formulas above is key to understanding how pressors work.
Source: GIPHY
The Sympathetic Nervous System versus the Parasympathetic Nervous System
Key to the idea of vasopressors is also getting an understanding of both the parasympathetic and sympathetic nervous system.
These are both involuntary (we don’t have conscious control over) nervous systems.
Source: GIFTenor
Let’s start with the sympathetic nervous system. The sympathetic nervous system goes a long way back. And I mean a long way. Thanks to this system, we weren’t eaten by dodos or sabertoothed tigers.
Source: GIPHY
Let’s go back in time and use an example:
I am a cavewoman I have been working hard all day putting some cool lil sketches on the wall of my cave (afterall, I do love home decor) and I am out taking an afternoon stroll. All of a sudden, I hear a loud scream and it scares the absolute shit out of me.
Source: GIFTenor
What’s going to happen to my body? How are my vital signs going to change?
Several things are going to happen in my body at once.
My heart rate? Skyrockets.
My blood pressure is going to go up.
My pupils are going to dilate.
The hairs on my neck and body are going to stand on end, and I’m going to start sweating.
In other words, I’m going to feel a surge of adrenaline. That surge of adrenaline is the same thing you feel when someone pops up and scares you, or if you think you are missing the last step on the staircase. Or if your husband surprises you by bringing home Taco Bell (just me? hello?)
My 30th birthday is coming up next month and this looks like a fantastic gift. Source: Facebook
All of the above actions fall under the category of the sympathetic nervous system – also known as our “fight or flight response”. The things above are going to help me out in the case that I either have to fight whatever is screaming at me or need to run away as fast as I can.
My HR increasing is going to increase my cardiac output (right? since CO = HR X SV)
The rise in BP is going to help perfuse all my organs and get more blood to the tissues that need it, especially the working skeletal music.
My pupils dilating will help me see better by letting more light into my eye.
The sympathetic nervous system’s goal is really to prepare the body for strenuous physical activity.
So here I am, ready to fight this thing, when out it pops out of the bushes:
Source: GIFER
Phew. No need to fight or flight. In fact, I can relax.
Cue my rest and digest nervous system – aka my parasympathetic nervous system. The parasympathetic nervous system will slow your heart rate, increase blood flow to your intestines and stomach to help digestion. The parasympathetic nervous system is responsible for – what I like to call the itis (if you don’t know what that means, check it out on urbandictionary.com – it’s what I get s/p Taco Bell meal). The parasympathetic nervous is definitely not the star of our vasopressor talk today but just an FYI that it does in fact exist and it is a thing.
The neurotransmitters that run the show: our catecholamines
Now that we’ve talked a little about our two main types of nervous systems, let’s move on to some more specifics.
Our body regulates itself by using two main things: ligands and receptors.
Source: KhanAcademy
Ligand is just a fancy name for a molecule that binds to a receptor. That molecule can be anything – hormones and neurotransmitters are examples of ligands that we produce endogenously (make it ourselves), whereas drugs are ligands that we give exogenously (from an outside source).
Receptors are located throughout our body – on every single type of tissue you can imagine. Receptors are all different chemically/structurally, so only certain ligands can bind to certain receptors. A receptor is just a molecule in a cell membrane that responds in a certain way to a ligand. In other words, when a ligand binds to a receptor, something is triggered/stimulated and something happens as a result.
Phenylephrine to the alpha-1 receptor. Source: GIFTENOR
Sometimes the analogy of a lock and key is used, where the lock is the receptor and the key is the ligand. Depending on the shape of the “key” (or the molecular ligand), it may or may not fit in that lock and cause something to happen. The whole basis of drug discovery is to synthesize molecules that can fit into (or BLOCK) these receptors to get effects that we want in our patients.
Many of the ligands (aka our vasopressor drugs) we will be talking about today – norepinephrine, epinephrine, dopamine, and vasopressin – are all synthesized endogenously (aka our body already naturally makes these chemicals) – so we weren’t really reinventing the wheel when we created them. But these drugs are literally lifesaving and are used every single day in the hospital (and some even are available over the counter to help with other stuff like a stuffy nose or a bleeding booty).
The unfinished office setup with fish tank and all! Source: It me
STUDY BREAK TIME. Go and take a biobreak, a 5 min stretch or walk. Tell someone ya love them. Over here at my household, we’ve been working on setting up my home office. She’s not ready yet, but part of the office is going to involve a freshwater aquarium. I’ve invested a ton of time researching the nitrogen cycle and all the cool stuff that needs to happen in your tank as the bacteria establishes itself before you can even put the fish in. So far we’re on week 2.5, and I’m about halfway through setting the happy bacteria up.
My dogs heard that this bed is designed for 1 medium-sized dog and they said “challenge accepted”.
Back to it!
Receptor Overview
Our bodies have a variety of different receptors on their cell surfaces. A receptor is essentially a structure located on a cell surface that, when stimulated, performs an action.
There are literally like a bajillion types of receptors in our body, but today we’re going to focus on the key ones to understand in the world of pressors: today talking about the alpha receptors and beta receptors.
Medicine is pretty old school, so it’s not a surprise that some of the most important receptors in our bodies are named after Greek letters.
Alpha (α) receptors are key in the regulation of blood pressure. There are two main types of alpha receptors you should know: alpha 1 receptors (α1) and alpha 2 receptors (α2).
Check out that artery dilating and constricting! Source GFYCat
Alpha 1 receptors are found in vascular smooth muscle (aka the muscle inside of our blood vessels). When stimulated, alpha 1 receptors cause the smooth muscles in our blood vessels to contract. As those smooth muscles in the vessels contract, they will cause constriction of the vessel and cause the size of the vessel to narrow.
Test your knowledge: What do you think will happen to blood pressure when an alpha 1 receptor is stimulated?
Alpha 1 stimulation causes smooth muscle in the vessels to constrict, and decrease the size of the diameter of that vessel. As a result, the systemic vascular resistance will increase. By reducing the size of that vessel (just like when we reduced the size of that ending of the hose), we will cause an increase in blood pressure.
Conversely, if we block that alpha 1 receptor, we will see smooth muscle relaxation and vasodilation. This will cause a decrease in blood pressure.
Alpha 2 receptors are a little bit out of the scope of today’s talk, but they are found both in the brain and in the peripheral tissues. When stimulated, these alpha 2 receptors will decrease sympathetic outflow (aka decrease the fight or flight response) and lower blood pressure. Some drugs we may give to patients to treat their HIGH blood pressure include alpha-2 agonists (stimulators) like clonidine.
Alpha 2 can be a little tricky to remember in the beginning since stimulation of alpha 2 has the opposite effect of alpha 1 stimulation. Keep in mind that when alpha 1 is stimulated, you get a rise in BP, but when alpha 2 is stimulated, you get a decrease in blood pressure.
Beta (β) Receptors
Beta receptors are also part of the sympathetic nervous system (aka our “fight or flight” system); just like with our alpha receptors, the two primary subtypes to know for our pressor talk are beta 1 (β1) and beta 2 (β2).
The beta 1 receptor is located primarily in the heart. When the B1 receptor is stimulated, it increases contractility of the heart (inotropy) and increases heart rate. Think B for Beating.
Beta 2 receptors on the other hand are mostly associated with being the the smooth muscle of the lungs (bronchi). When stimulated, these bronchial muscles relax, and open up airways, making respiration easier.
Keep this in mind – this will come in handy as a way to remember a certain vasopressor later.
We love a good table to review:
Receptor Name
Effects whenstimulated
α1
vasculature vasoconstriction
α2
inhibition of neurotransmitter release (decrease of sympathetic tone)
β1
increase heart rate and force of heart contraction
β2
smooth muscle relaxation (e.g. bronchial/lungs)
Let’s finally talk about the first star of the show: phenylephrine.
Phenylephrine
Phenylephrine is a direct acting sympathomimetic amine (aka it’s a molecule that we created that mimics catecholamines and stimulates part of the sympathetic nervous system).
Source: Biomol GmbH
Phenylephrine is one of the unique pressors because it only hits one type of receptor – the alpha 1 receptor. Think about your receptors we learned about above – what effect would stimulation of the alpha receptor have? Would it: increase blood pressure? Increase cardiac output? Increase heart rate?
By acting on the alpha receptors, phenylephrine causes blood vessels to constrict – which then decreases the diameter of your vessels (aka also increase systemic vascular resistance or SVR) and ultimately increases blood pressure.
By causing arterial vasoconstriction, phenylephrine increases afterload (don’t know what the heck I’m talking about? Check out this talk here).
Because phenylephrine only works as an alpha-1-agonist (stimulator), it has no direct effect on heart rate – it will not cause an increase in heart rate. In fact, you might actually see the opposite effect and see bradycardia or a slow heart rate. Can you think about why that may be?
Source: GIFTenor
Hint hint – remember your blood pressure formula!
Keep in mind that oftentimes, your body likes to compensate for abrupt changes.
Since BP = CO x SVR, and you are increasing SVR, your body might respond with a decrease in cardiac output, or CO.
If you remember – cardiac output is the amount of blood our heart pumps out per unit of time, or SV (stroke volume) x HR (heart rate).
Your heart isn’t great at abruptly changing stroke volume, but what it can do, is quickly change HR. To decrease cardiac output, your body will respond by a decrease in heart rate – bam, bradycardia – or more specifically, reflex bradycardia.
Formulations
Phenylephrine is given via IV continuous infusion with a bag or it is also available to give as a push dose via a stick (typical push dose ~50-200 mcg per push, repeat q 2-5 min).
The bag version – the type we’d use for a continuous infusion. Source: SteRX
Phenylephrine sticks should be very carefully monitored for a multitude of reasons. A big one is that a phenylephrine stick has a concentration of 100 mcg of phenylephrine per mL and is available in 10 mL or 5 mL.
So, how many total mcg are available in either syringe?
Well 100 mcg/1 mL = “X” mcg/5 mL; X = 500 mcg total (5 mL syringe); 1,000 mcg total (10 mL syringe).
So what happens if you have a patient get hypotensive (low blood pressure), and you push the whole thing into a patient? Woof.
That stick should be watched very carefully and used by someone who is familiar with its dosing, since it is very easy (and scary) to just pop in the whole thing – after all, it’s only 5 or 10 mL, and we often give 10 mL normal saline flushes like they are no big deal. Instead, doses like HALF A ML (0.5 mL) up to 2 mL (50-200 mcg) should be given every 1-5 min.
Also keep in mind that phenylephrine is fast on and fast off -it starts working within ~1 min and can last up to 20 min (but realistically we see it start to drop off after 5 min) so if you expect that your patient is going to stay hypotensive, you’re going to have a make a drip (aka a bag and start a continuous infusion) anyways; the push dose is just to hold them over.
The Phenyl stick *BUM BUM BUMMM*. Source: Academic Life in Emergency Medicine
Keep in mind that the perfect titratable drug to give via continuous infusion is one that is fast on/fast off. Fast on means that it will start working quickly – very much desired for our BP-crashing patients. Fast off – though it might sound bad because we don’t want the effects to go away “per-say” is actually also very desirable. This means you can quickly increase or decrease the rate of the drip/continuous infusion and not have to worry about things like accumulation.
Also can do non-weight based dosing, though weight based seems to be the most prevalent
IV push/phenyl stick (phenylephrine)
50 mcg – 200 mcg bolus over 20-30 seconds
Usually available in 10 mL syringe (conc 100 mcg/mL) – do not push whole stick (!)
When to Use:
Every patient is different, but in general – we like to use phenylephrine when your patient has hypotension with tachycardia – since it does not increase HR like a lot of our other pressors can. We also like to use phenylephrine in patients with normal cardiac function (since it doesn’t add any support because it doesn’t hit beta-1).
It can be used in things like refractory afib with rapid ventricular rate (RVR), or in septic shock, neurogenic shock, and hemorrhagic shock – assuming that you’ve first replenished volume in the vessels first if needed. (Keep in mind – if your patient is bleeding out to death – you can squeeze and clamp down those vessels all you want – but without enough volume, you won’t get a good enough BP/perfusion). It can also be used in intra-op hypotension and hypotension seen with anesthesia.
It’s not the most commonly used pressor (even in the indications above), but it definitely has its place.
Source: GIFPHY
Question (for those who have reviewed the heart failure section already): Is phenylephrine a good pressor choice in those with systolic heart failure? Why or why not?
Phenylephrine is definitely not the pressor of choice in systolic heart failure. Keep in mind in this condition you already have a weak, tired, left ventricle. Yes, he contracts and tries, but he’s super super weak and can’t generate a large force of contraction to PUSSSSSHHHH that blood out. The last thing we’d want to do in this patient is add on an agent that solely increases afterload. By increasing the pressure in the arteries and increasing the amount of pressure that LV now has to push against, that’s like saying “hey I know you’re really weak and tired but can you actually push harder?”
Source: GIPHY
The same is true in cases of severe pulmonary hypertension – something we haven’t discussed yet – avoid phenylephrine in these patients.
Key Side Effects:
Source: GIFTenor
Reflex bradycardia, like we discussed above.
High blood pressure (aka hypertension). Obviously one of the reasons we are using it as a pressor, but may not be wanted if we are using it for a different indication. This is a potential side effect of any pressor that also hits alpha-1 receptors.
Anxiety, headache, restlessness, insomnia, excitability (hi, it me). Not surprising given that phenylephrine is a synthesized catecholamine. This is a potential side effect of any pressor that also hits alpha-1 receptors.
Ischemia (aka inadequate blood supply) which can lead to tissue death if not fixed. This is pretty much true of any pressor that works on alpha-1 receptors. Besides vasoconstricting our large arteries, they also vasoconstrict smaller vessels like those in our fingers, toes, blood vessels feeding the gut, etc. The vasoconstriction of these smaller vessels leads to an overall decreased blood flow to the tissue they support, so we can see things like gut ischemia, digital (finger) ischemia with long term or high dose vasopressors. In medicine though, everything is, of course, risk versus benefit, and phenylephrine is one of our life saving medications. This is a potential side effect of any pressor that also hits alpha-1 receptors.
Sorry I didn’t warn ya – Digital Ischemia caused from a vasopressor. Bet you won’t forget it now! Source: Cureus
Tissue necrosis if phenylephrine infiltrates your peripheral line (aka the medication starts leaking out of the vein/vessel at the injection site). This is why we give all of our pressors through central lines, which are stronger and terminate in a large vein causing rapid and good dilution of the drug. However, you never want to delay pressor administration due to lack of a central line. This is a potential side effect of any pressor that also hits alpha-1 receptors. If you do see infiltration, phentolamine can be used as a treatment. Phentolamine is an alpha receptor antagonist so it can counteract the effects of phenylephrine. You can dilute 5-10 mg in 10-20 mL NS and administer to the site of extravasation and repeat PRN.
A key thing I wanted to quickly mention: cardiac arrhythmias are not common with phenylephrine.This is because phenylephrine does not hit the beta-1 receptor. This is not true of some other pressors we will eventually talk about!
FYI: Other uses
Because of its effects on constricting blood vessels, phenylephrine can also be used more locally (not systemically) to treat other conditions such as hemorrhoids (caused by dilated/swollen veins in the rectum), as a nasal spray decongestant (constricts blood vessels in the nose, to treat intraocular bleeding, and to treat priapism (which is when the penis remains erect for hours – super dangerous since the blood that remains in that penis is sitting there and starts getting deprived of oxygen). We literally inject (with a needle) phenylephrine right into the penis (in an area called the corpus cavernosum) to help restrict those blood vessels and decrease blood flow into the penis. I’ll never forget when I was a resident and I heard an unlucky patient go through this procedure. Terrible, but better than the alternative which is possibly losing some or all of your penis due to tissue death.
Fun fact for my pharmacy-interested friends: trazodone (or “trazobone” as we say in the business) is a possible cause of priapism.
Fun fact – if phenylephrine can be used to stop erections, what do you think can be given orally to help patients get an erection? *hint: we’ve already talked about it today briefly*
[ insert thinking pause here ]
Phentolamine – our alpha antagonist.
It can also be used locally in the eye (via drops) where it constricts the dilator muscle causing dilation of the pupil – making fundoscopic exams possible.
Stay tuned for more fun, less priapism-related pressor talk in future posts! Stay cool.
Today we’re talking rhythm control (it’s kinda a doozy, sorry in advance, love u). In order to get the most of out today’s talk, I recommend these previous “pre-readings” of sorts:
Rhythm control is when we attempt to not only convert a patient back into normal sinus rhythm but also to maintain that sinus rhythm. Unlike rate control, a patient that undergoes successful rhythm control is no longer in afib.
What are the ways we can obtain rhythm control in our patients?
There’s a bunch of different ways to try and achieve rhythm control in afib. These include ⚡electrical cardioversion ⚡, antiarrhythmic drugs 💊, radiofrequency catheter ablation 💥. It’s not uncommon to also use a combination of the above approach.
What is ⚡electrical cardioversion⚡?
The word cardioversion refers to the conversion of an abnormally fast heart rate (aka a tachycardia) to a normal rhythm. It’s important not to necessarily mix up the term cardioversion to only mean electrical cardioversion. Cardioversion can also be achieved by the use of medication.
When referring to electrical cardioversion, we are talking about using a therapeutic dose of electrical current directed at the heart.
Source: GIPHY
In the treatment of afib, we use something called synchronized electrical cardioversion. In synchronized electrical cardioversion, we apply the shock at a specific moment in the cardiac cycle.
Source: GIPHY
Why?
Well, if you remember back to our cardiac action potential – our P, QRS, and T waves – you might remember that there is something called a refractory period – this happens after the original impulse is sent to the ventricles and as our myocardial cells are repolarizing and relaxing.
Source: Knowledge of EKG via Facebook.com
Let’s review it: an electrical impulse gets sent to the ventricular cells – the impulse stimulates a depolarization or contraction. But during repolarization, we have a refractory period.
If you try to dust off the dusty cobwebs of the corner of your brain from college, you might remember that a refractory period is a period of repolarization where a muscle is relatively unresponsive tofurther stimulation.
The refractory period is made up of two different phases: the absolute refractory period and the relativerefractory period.
During the absolute refractory period – NO stimulus, no matter how intense, can stimulate another new action potential.
However, during the relative refractory period, if a stimulus is STRONG enough, a new action potential may be triggered.
Source: GIF Tenor
This period of relative refractoriness corresponds with the t-wave peak (apex) on the EKG.
Why is this bad?
Let’s say your patient is in afib and you accidently deliver an uncoordinated shock and it shocks the patient at the peak of that T wave – during the relative refractory period…
Source: GIPHY
That shock may induce a separate stimulation of the ventricles, causing an early ventricular depolarization. Often this is seen as a premature ventricular beat (aka PVC) that can induce disruption of the ventricles but can also lead to ventricular fibrillation (aka a cardiac arrest). Not good.
Source: GIPHY
For this reason, we use synchronized cardioversion to avoid shocking during this period of vulnerability and instead synchronize the shock with the QRS complex – when the heart is at its least vulnerable.
The machine will spit out 120-200 joules of energy to stop the afib and convert your patient to normal sinus rhythm (hopefully).
Another common misconception I get from learners is that the shock causes the afib to just morph into NSR. The truth is a little different.
Cardioversion actually resets the heart. It upsets and stops the abnormal signaling in the hope that the heart will reset back into normal sinus rhythm. It’s like resetting your computer – you have to stop it and shut it down in order for it to reset.
Source: GIFTenor
⚡Electrical cardioversion⚡ is a reasonable first line option for patients who are pursuing rhythm control. If that fails, often times we will try the combination of both antiarrhythmic medications to “prime” your patient and help them successfully convert with electrical cardioversion.
We also opt to use electrical cardioversion in the acute setting when patients present with a rapid ventricular rate response to AF and are hemodynamically unstable.
Keep in mind that electrical cardioversion is NOT only used in the acute setting. Like I said before, it’s a reasonable first line option for any patient pursuing rhythm control.
Oftentimes we will schedule a cardioversion for patients and have plenty of time to give them sedation and pain medications to make the process go as smoothly as possible.
Source: GIPHY
Always remember that cardioversion has some specific anticoagulation requirements with it (mentioned in the pre reading).
The longer you have afib, the more structural damage that happens to the heart as that ventricle beats faster. This is why past a certain point, especially in older patients with structurally damaged hearts, their afib becomes permanent.
Source: GIPHY
We can still try cardioversion in patients with persistent (not PERMANENT) afib, provided that it converts them for a clinically meaningful time between procedures. Once a patient has permanent afib, we no longer will try any rhythm control method, including cardioversion, since it is unlikely to be successful.
Source: GIPHY
💊Pharmacological Cardioversion💊
Like I said above, drugz can also be used to cardiovert your patient. They can either cardiovert the patient in and of themselves or be given to help the effectiveness of electrical cardioversion.
Protip: pharmacologic cardioversion is most effective when started in the first week after an episode of AFib started.
The other thing I think is also often forgotten is that there are different antiarrhythmic drugs used for cardioversion of afib versus for the maintenance of afib. Yes, there is some overlap, but some drugs that are used for maintenance are not used for conversion and visa versa.
Now, I’ve thought long and I’ve thought hard of ways to simplify what can be used for what. She’s not perfect, but the below is what, when in doubt, I personally use to help remember :
Now let’s talk about efficacy and practicality (and, you know…what data we actually have on these agents). Again, these are the meds we can use for cardioversion: our “DIP-AF” meds.
Pharmacologic Conversion: Ibutilide
Source: RK.md
Ibutilide is one of our IV options for pharmacologic conversion of AFib and is decently effective, with an efficacy rate of about 50% of the time when given in those with recent-onset afib with an average conversion time of <30 minutes.
These patients will get 1 mg of IV ibutilide over 10 mins and can get a repeat 1 mg one more time if needed (if your patients are small, <60 kilo, opt for the 0.1 mg/kg dosing instead).
Pretreating with ibutilide prior to electrical cardioversion also improves the likelihood ibutilide will work.
The biggest risk of giving ibutilide is QT prolongation as it can cause Torsades de Pointes (aka TdP), with an incidence of ~3-4%.
Patients who receive ibutilide have to be monitored via EKG for at least 4 hours post administration and have resus equipment nearby in the case that your patient is in that 3-4% and deteriorates further into a cardiac arrest.
Avoid in patients with severe hypokalemia, QT prolongation, or an ejection fraction less than 30% (all due to increased risk of ventricular proarrhythmia in these patients). Some people advocate to give some IV magnesium sulfate prior to ibutilide to help decrease this risk.
So overall (the TLDR version): ibutilide works decently if your patient is a candidate but a big con is that you need to monitor the patient for 4+ hours as it has a high risk of QT prolongation/TdP so may not ideal in an ED setting, for example.
Propafenone and flecainide are pretty cool options for patients with afib that are candidates for them. They are known as pill in the pocket therapy. This is basically for patients who can tell/feel when they are in afib.
Propafenone. Source: GoodRX
With these therapies, they don’t have to take a maintenance antiarrhythmic everyday.
However, when they feel that they are in active afib, they can take their propafenone (or flecainide) pill out of their pocket and take it in that moment to restore normal sinus rhythm again.
Because this is technically an outpatient therapy that the patient will take on their own – and cardioversion has risks involved with it – like bradycardia, AV node dysfunction, or having a proarrhythmic response – we always like to do an initial conversion trial in a monitored setting to make sure this therapy is safe and effective before sending these patients out into the wild to take on their own.
Pharmacologic Conversion: Amiodarone
Source: GoodRx
Amio is ….eh, kinda unimpressive by itself. We know amio has some beta blocking effects which make it good for lowering a fast ventricular rate, but it’s antiarrhythmic properties in the cardioversion setting…are not that great in the sense that they take a while to work (time delayed). Data shows that when oral amiodarone was loaded over the course of several weeks, only about 25% converted to sinus rhythm. Oral amiodarone can be used for cardioversion in a less acute setting, and is a reasonable option, but if you want a quick cardioversion…probably not your best bet.
Protip: the easiest way to remember your special “pill in pocket” drugs is to remember they are both class 1c antiarrhythmics.
Can’t get your class 1 antiarrhythmics down? I always recommend reverting back to the age old mnemonic:
Now, I used to know this whole burger thing and it was helpful but for some reason I always forget what came second: is it the fries? Do I add mayo now?
Source: GIPHY
But the trick that always helped me was to remember: always finish making your burger FIRSTbefore moving onto the sides (aka the fries please).
Speaking of our 1Cs (our pill in pocket therapy – our fries, please – propafenone and flecainide), you do not want to use these agents in patients with a hx of coronary artery disease (CAD) and structural heart disease.
The history of why is pretty interesting.
Source: GIFER
I think that it’s so easy to learn cardiology today and be like “OK and we don’t use these agents in XYZ” and think that we’ve always known these things.
Because medicine is so all-knowing and smart right?
Source: GIF Tenor
The truth of medicine is that it takes a lot of trial and error, and good hypotheses don’t always lead to good outcomes. And in those cases….you live and you learn. And you’ll see what I mean.
Let’s take it back to 1991. Paula Abdul is on the radio.
Source: GFYCat
The healthcare community had been noticing that patients that are status post myocardial infarction (aka after a heart attack) tended to have an increased incidence of premature ventricular contractions, aka PVCs.
PVCs are pretty common, even in you and me, and is the name for when a heartbeat is initiated in the Purkinje fibers in the ventricles rather than the normal SA node.
Usually they do not pose any danger and may either be completely asymptomatic, they may also be perceived as an “extra heartbeat” or a palpitation.
Have you ever just been chilling watching a show or reading a book and all of a sudden you feel your heart beat and pound for a couple beats?
……..
No?
Just me?
Well whatever, if so, what you’re probably experiencing is a PVC.
Anyway, back to our 1991 trial – the CAST Trial – aka the Cardiac Arrhythmia Suppression trial. They noticed that patients s/p MI had an increased incidence of PVCs and investigators asked – if we suppress these excess ventricular ectopies in these patients – can we reduce the incidence of more severe ventricular arrhythmias and reduce sudden death in these patients?
Ok cool cool, so they randomized patients that were anywhere from 6 days to 2 years after their MI, had a lower EF (55% or less if within 90 days post MI or 40% or less if recruited >90 days out) and were randomized to either placebo or encainide (no longer on the market but was also a 1c agent) or flecainide.
We were hoping to see a decrease in mortality, save the day, and prevent death in our vulnerable post MI patients.
But…..
Instead…..
We had to stop the trial early.
Because, even though we suppressed these PVCs, we also found that our 1c agents significantly increased the rate of death and cardiac arrest (over 2.5x!) with a number needed to harm of 29 during a follow up period of only 10 months.
In other words, in less than a year, for every 29 patients you treated with a class 1c, you caused a death.
NOT. GOOD.
Source: GIPHY
Thanks to this trial, class 1c agents are now contraindicated in patients with coronary heart disease or structural heart disease.
The other thing to know: when using a class 1c agent (aka flecainide or propafenone), your patient must first be on an AV-nodal blocking agent (e.g. a beta blocker, or non-DHP calcium channel blockers).
Why?
Our class 1c agents are able to slow down the atrial rate. That may sound good, but if the rate slows enough, you can end up with 1:1 AV conduction and an increased ventricular rate as a result. This is because even though these agents are slowly down atrial rate, the atria is still firing at a rate higher than what is normal, and can cause ventricular tachycardia if conducted 1:1.
Maintenance of Normal Sinus Rhythm and Prevention of AFib Recurrence
Ok, so we snapped our patients out of Afib, either with some electricity or some drugz or a combo of both.
Now we have to give meds to keep your patient in NSR and prevent them from going back into afib.
Cue the infographic again:
The following can all be used for maintenance of NSR, depending on patient specific factors: amiodarone, flecainide, dofetilide, dronedarone, disopyramide, propafenone, sotalol and quinidine.
However, our class 1a agents (disopyramide and quinidine) for AFib have been associated with a possible increase in mortality, so aren’t commonly used and not included in our first-first line options. Amio is also usually reserved for further down the line if possible due to long term adverse effects.
Drug selection for antiarrhythmics is driven to a greater extent by safety concerns than it is by drug efficacy.
Even the AHA guidelines say “a common approach [to finding the best agent for your patient] is to identify available drug choices by first eliminating…drugs that have absolute or relative contraindications.“
Does your patient have structural heart disease? Do they have coronary artery disease? Do they have heart failure or LV hypertrophy? Do they have risk factors or other meds that can cause QT prolongation? How’s their renal or hepatic function? These are all things that are going to help you narrow down what agents you can even use.
Efficacy:
With the exception of amiodarone which tends to be the most effective agent, the majority of the maintenance antiarrhythmics have an efficacy rate of about 30-50% at 1 year.
Specific Agent Review
Normal Sinus Rhythm Maintenance: Amiodarone
Because of its long term toxicities to almost every organ ever (jk but not really), amiodarone should only really be used after other agents have failed and/or are contraindicated. Amio is a pretty dirty drug in that it hits multiple ion channels – Na, K, Ca, and also has better blocking properties. It also has a super long half life and distributes widely into adipose tissue. Amio tends to take days to weeks to have its antiarrhythmic effect and QT prolongation. If you “load” with amio (aka give higher doses in the beginning to reach steady state faster) , you can accelerate its onset of activity. Amio also has a lot of drug-drug interactions because it inhibits liver enzymes CYP3A, CYP2C9 and also P-glycoprotein, so can mess with the metabolism of other drugs like warfarin or digoxin. When in doubt, DDI checker-it-out. In terms of long term efficacy for maintenance of sinus rhythm, amio is actually pretty damn good. In patients with paroxysmal or persistent AF, it performed better than dronedarone, sotalol, and propafenone.
Amiodarone. Source: Wikipedia
The biggest CV side effect of amio is bradycardia. Even though QT prolongation can occur, we almost never see it inducing Torsades de Pointes. Because of its long term toxicities (thyroid, liver, ocular, dermatologic, pulmonary, etc), we don’t like to use it first-line, especially in younger patients when we have other options. Many toxicities are dose-rated but can be fatal. To prevent this, lower oral doses of <200 mg PO QD can be given chronically and may still be effective and have less side effects. Obviously, routine surveillance of these organs should be done. In those with LV hypertrophy, HF, CAD, and/or previous MI, amiodarone has a low risk of arrhythmias, make it a good initial agent in these patients.
Normal Sinus Rhythm Maintenance: Flecainide and Propafenone
Remember, ladies and gents. Source: Candy Doll Club
I’m just going to group these two together here. If you remember from above, these are our Class IC drugs (Fries Please!) and (if you also remember) can only be used in patients with AF without structural disease. Flecainide and propafenone also have negative inotropic properties (decrease the force of contraction of the ventricles) and should be avoided in those with LV dysfunction. As we said above, these agents have to paired with AV nodal blockers due to the risk of atrial slowing causing 1:1 AV conduction. These agents can also cause up to a 25% increase of the PR and QRS intervals – but when a greater increase is seen in the QRS duration, it may be a marker for proarrhythmia risk. Use caution with these agents in patients with significant conductions system disease. Both agents are pretty well tolerated and if they do cause side effects, though uncommon you can see dizziness or visual disturbances with both and a metallic taste with propafenone. Both flecainide and propafenone have beta blocking properties, but their metabolites are electrophysiologically active with weak beta blocking properties. This might come in handy to know especially when it comes to propafenone and CYP2D6 – propafenone is a substrate of CYP2D6 – up to 7% of patients do not possess CYP2D6 (we call these peeps poor metabolizers) – and other drugs such as antidepressants, quinidine, fluoxetine, etc can also inhibit this enzyme leading to more than expected beta blockade.
Normal Sinus Rhythm Maintenance: Sotalol
Sotalol. Source: GoodRx
Sotalol: If you noticed in the infographic, sotalol is one of the agents that is not used for cardioversion but can be used for maintenance of NSR. This is because it is ineffective for pharmacologic conversion but does serve a role in maintaining that NSR. The important thing to remember with sotalol is that it can cause QT prolongation and TdP (a pretty high risk compared to our other agents) and also that it is renally cleared. Because of this, it should either used with caution or outright avoided in patients with chronic kidney disease or unstable renal fxn. Because of its high risk of QT prolongation and TdP, it used to be required to be initiated in the hospital setting. Even though its not required anymore, I’d say a lot of providers still initiate it in an inpatient setting and monitor EKG for QTC prolongation for the first few days of therapy. Make sure to periodically monitor potassium, magnesium and renal fxn in patients on sotalol.
Normal Sinus Rhythm Maintenance: Dofetilide
Source: SIgmapharm Labs
Dofetilide is one of our class III (K blocking) antiarrhythmic agents.
Because of the risk of QT prolongation with this drug, it is only considered for rhythm control in patients who are deemed low risk for torsades de pointes due to QT prolongation.
Dofetilide is pretty well tolerated and has very minimal non-cardiac side effects. Besides amiodarone, dofetilide is one of our more efficacious agents – one trial showed that it had a 58% efficacy of maintaining NSR at 1 year post cardioversion (with a 0.8% incidence of Torsades). In another trial of patients with HFrEF, it had an efficacy of 79% at 1 year in maintaining NSR.
Source: SBS
Like sotalol, it has that high risk of QT prolongation, and it is still mandatory to initiate this agent in an inpatient setting when either 1) initiating therapy or 2) escalating the dose. I remember seeing my first dofetilide patient in the hospital during my clinical student rotations. He was just a “normal” looking guy – not sick, not fatigued, not anything – that in any other scenario, would not be in the hospital. But he just had to chill out in his hospital bed and sit there while we started his dofetilide therapy – he’d take a dose, get his EKG monitored – and then sit and watch movies until his next dose. Just like sotalol, dofetilide is also renally adjusted, dosed by CrCl, and dose adjusted and/or discontinued based on the degree of QT prolongation.
Normal Sinus Rhythm Maintenance: Dronedarone
Source: IndiaMART
Dronedarone: You might be asking yourself – why does this drug sound suspiciously like amiodarone? It’s because it’s an analog of it – and lacks its iodine moiety. Because of this, dronedarone is better tolerated and has less side effects than amiodarone.
Even though it’s better tolerated than amiodarone, it’s also much less efficacious. Dronedarone should not be used in patients with HFrEF because it was found to increase the likelihood of stroke, MI, embolism or CV death. It should also not be used in patients with NYHA class III or IV HF and in patients who have had an episode of HF decompensated within the past 4 weeks, especially those with low EF.
Dronedarone is also a messy drug like its cousin amiodarone, and also has beta, sodium, calcium, and potassium blocking properties. Although it has a lot fewer side effects compared to amiodarone, it can still cause bradycardia and QT prolongation. Torsades de Pointes is rarely seen with dronedarone (just like amiodarone) but it has been reported.
Just like amiodarone, it has multiple drug-drug interactions with CYP3A4, CYP2D6, and PGP so again, this is one agent you’ll want to run a DDI checker on. Unlike amiodarone, dronedarone does not alter the INR when used with warfarin.
Even though we spared some of amio’s gnarly side effects like dermatological, ocular, and thyroid toxicity, we still can see hepatotoxicity during the first 6 months of therapy – so liver function tests should be done, especially during these first 6 months.
Normal Sinus Rhythm Maintenance Misc: Disopyramide + Quinidine
Source: Green Pharmacy
Disopyramide: Also one of the agents that is not used for cardioversion, disopyramide is a sodium blocker that has both anticholinergic and negative inotropic effects and can be used for maintenance of NSR in patients with afib, and is used after electrical cardioversion to keep patients in NSR. Disopyramide is unique in that it has anticholinergic effects, and because of these effects, it can be useful in patients that experience their AFib during times of high vagal tone – like during sleep, coughing, straining etc. Because of its negative inotropic effects though, it should be avoided in those with structural heart disease. All in all, it isn’t used super commonly since there is a systematic review that suggests it may increase mortality slightly (along with quinidine).
Source: Green Pharmacy
Quinidine: One of the Na blockers (class 1 agents), quinidine also has K channel blocking effects at slower heart rates as well as vagolytic and alpha blocking properties. This drug is old and was one of the first used to ever treat AF. You don’t usually see it that often because, like disopyramide, has been associated with a slight increase in mortality. It can prolong the QT interval, can cause Torsades, and isn’t used frequently. The (one?) pro about quinidine is that it can be used even during advanced renal dysfunction. If starting your patient on quinidine, you’ll need close EKG monitoring d/t the risk of TdP. TLDR: quinidine is old, not used often, and if you’re using it, it’s probably because you can’t use any of the newer agents.
My patient is pursuing rhythm control but occasionally has infrequent spells of AFib. Do I give up or switch?
Nope! Often times patient symptoms may improve even without complete AF suppression. If you can get your patient from frequent, symptomatic bouts of AFib down to infrequent, well-tolerated bouts of AF – that’s a totally reasonable outcome – and does not necessarily mean you have to stop therapy.
If my drug requires EKG monitoring for initiation, when do I take the EKG?
Source: GIPHY
Like discussed above, a lot of these antiarrhythmics are also proarrhythmic. Many of them carry with them a risk of QT prolongation and TdP (cough cough dofetilide and sotalol) and QRS prolongation (cough cough flecainide and propafenone). The optimal time to perform the EKG is when whatever drug you are using reaches peak drug concentration. So check the pharmacokinetics of your particular drug and go off of that.
When to do rhythm over rate control?
Difficulty in achieving adequate rate control
Younger patient age
Symptomatic despite adequate rate control
Tachycardia-mediated cardiomyopathy (aka ventricle goes boom boom too often and now your heart is enlarged and unhappy)
First episode of AF/early AF (why? less structural damage)
AF precipitated by an acute illness
Patient preference
When definitely not to do rhythm control:
When the patient’s afib has been deemed to be “permanent”. Don’t risk bad side effects for no reason, dawg.
In patients with history of syncope, sinus bradycardia, PR interval prolongation (aka AV node issues), bundle branch blocks…we get a little bit more concerned with the risk of bradyarrhythmias with our agents
Big Takeaways for our Antiarrhythmics:
Different agents exist for maintenance versus cardioversion.
Cardioversion agents:
Dronedarone, ibutilide, propafenone, amiodarone, and flecainide can all be used for pharmacological conversion of AF, provided contraindications to the select drug are absent.
Amiodarone is an acute crummy cardioversion agent but can be good acutely for its rate controlling properties.
Propafenone and flecainide can be given as “pill in pocket therapy” and are both class 1c agents.
Do NOT use the pill in pocket therapies for patients with coronary artery disease and structural heart disease.
Maintenance Meds
Drug safety, not efficacy drives selection.
Check out the below to help guide you in your selection (zoom in to see better)!